Using a Genomics Taxonomy: Facilitating Patient Care Safety and Quality in the Era of Precision Oncology
Oncology nurses need to be competent in the ever-expanding application of genomics in cancer care, and understanding foundational terms is necessary. A landscape analysis of Oncology Nursing Society (ONS) materials, a literature review, and expert opinion revealed inconsistencies and varying use of genomic terms, some of which are outdated. In response, the ONS Genomics Taxonomy was built to address inaccuracies and discrepancies in terms and to be an accessible resource for oncology nurses. The taxonomy is a living document that is updated to reflect evolving science and evidence and serves to diminish confusion, improve genomic literacy, and assist oncology nurses in providing safe genomic care.
AT A GLANCE
- Advancements have transformed cancer care from genetics into genomics, necessitating changes in terminology used by professionals to avoid confusion and reflect the current state of the evidence.
- Patients and families rely on nurses to explain genomic terminology and concepts in ways that can be easily understood, which is facilitated by a taxonomy.
- Oncology nursing education programs should use consistent, accurate, and current terminology when providing education on genomic concepts.
Jump to a section
Genomics is fundamental to cancer care and foundational to oncology nursing practice. However, practicing oncology nurses’ knowledge of genomics is limited, and few oncology nurses have learned genomic content during educational preparation (Aiello, 2017). Expanding implications for germline genetic testing (Giri et al., 2020), as well as the rapid influx of biomarkers, biomarker testing with new technologies, and targeted therapies into cancer care, necessitate use of accurate and consistent terminology reflecting current evidence. Understanding these foundational terms and concepts is critical to reduce errors and confusion in practice and increase quality of care. The many quality and safety implications to genomics-based oncology care include incorrect or no somatic and/or germline testing performed when indicated; missed or incorrect genetic professional referrals; test result misinterpretation, leading to incorrect or absent interventions and/or therapies; and patient and family confusion—all of which result in missed opportunities for cancer prevention and effective cancer treatment.
Terminology is transitioning in cancer care from genetics into genomics as technology and science evolve and evidence-based testing applications expand. Genomics, the entire genome of any organism (including humans), is an expansion of genetics, which refers to a specific gene, such as BRCA1 (National Human Genome Research Institute, 2020b). The focus on genomics is largely the result of rapid advances in technology, with substantial reduction in costs. The benchmark, now largely achieved, has been the ability to sequence an entire genome for $1,000 (National Human Genome Research Institute, 2020a). This was a cost considered within range of other healthcare tests that would make it feasible to translate genomics into practice to improve health outcomes.
As a result, patients with cancer receive increasing amounts of individualized genomic information about their disease through germline and somatic biomarker testing. The varied and inconsistent use of terms is a definite obstacle to effective patient–clinician communication and, ultimately, to optimal patient care (Martin et al., 2020). Oncology nurses play an essential role in leading the patient and family through the complex matrix of tests, results, and therapy plans. The development and adoption of a standard taxonomy improves communication among healthcare professionals, helps nurses educate patients and their families, diminishes confusion and the risk for error, and reflects the current state of the evidence.
Genomics Through a Quality and Safety Lens
The risk for error because of lack of genomic literacy is best illustrated by a case study of a nurse and other healthcare providers who appear to have misinterpreted the results of a germline genetic test, resulting in the patient undergoing risk-reducing surgery that was not indicated based on the genetic test results (Ray, 2017). The patient’s genetic testing result, a variant of uncertain significance (VUS), illustrates how important terminology is to the provision of quality health care. The genetic test was abnormal because a VUS was detected. A VUS is considered a mutation according to the definition of a mutation being a change in a DNA sequence (National Human Genome Research Institute, 2020b). However, mutations are not all the same; they can be benign (harmless with no effect on gene function) or pathogenic (altered gene function that contributes to disease development). The outdated term “mutation” connotes harm, but in this case of a VUS, the evidence was insufficient to determine whether this genetic change altered the function of the gene or had any health implications. Confusion about the meaning of the term “mutation” is partially why the American College of Medical Genetics changed the nomenclature to increase clarity (Richards et al., 2015).
The patient also did not understand the genetic test results; she thought her results were “positive” and either failed to understand or was not counseled on the meaning of a VUS, leading to unnecessary surgery (Bever, 2017). Many healthcare providers aside from the nurse were involved in the care of this patient. The important point is not to define whether someone is or is not at fault; the point is that terminology and language matter to healthcare quality and safety, and many healthcare providers are unfamiliar with genomic terms. A study by Macklin et al. (2019) demonstrated that almost half of surveyed physicians (n = 39 of 84) incorrectly defined a VUS in a case study scenario. Proper classification of genomic variants and level of variant pathogenicity is critical for safe genomic care. The use of consistent and accurate terminology reduces medical errors and facilitates effective patient and family education and comprehension of complex genomic concepts (Haga et al., 2014; Kohn, 2001). Foundational terms and a taxonomy of key concepts are the essential underpinning for improving oncology nurse genomic competency. There is ample literature describing adverse events that can occur due to lack of genomic literacy (Bonadies et al., 2014; Brierley et al., 2012; Farmer et al., 2019; Mahon, 2019).
Objectives and Methods
In 2019, the Oncology Nursing Society (ONS) established a Genomics Advisory Board (GAB) of genomic nursing experts who conducted a membership survey to inform genomic action items, and they found that term definitions were needed. A GAB knowledge project group was established and charged to develop genomic education. The work could not move forward without setting foundational terminology to be used consistently throughout educational offerings and resources. This group (a) identified terms that required definitions based on the survey; (b) performed a landscape analysis of current ONS materials and expert input; (c) used established peer-reviewed definitions; (d) identified companion graphics; (e) created clinical examples; and (f) categorized terms based on use in practice. The resulting taxonomy then went through peer review with the entire GAB.
Formulation of the Taxonomy
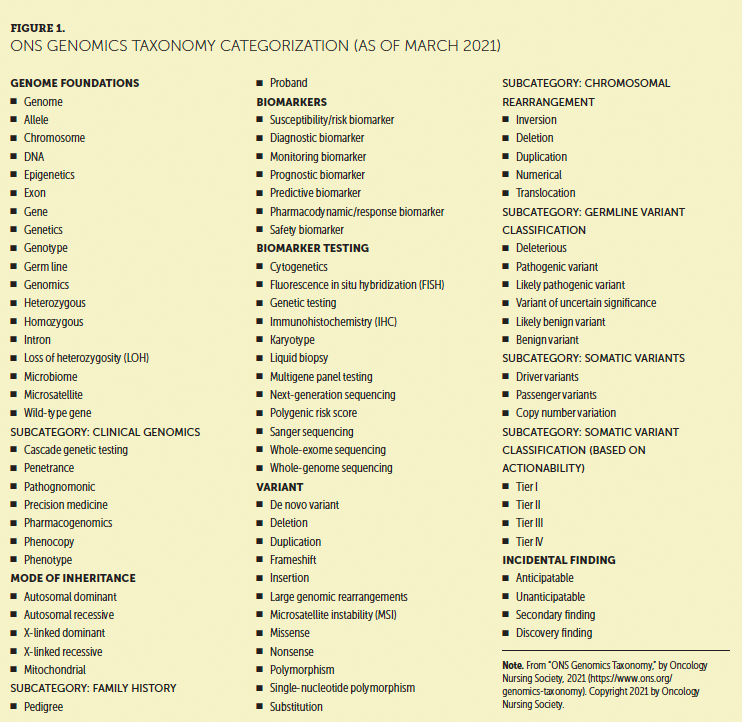
Identifying and defining genomic terms quickly illustrated the need to group or classify terms based on subject categories, and the taxonomic structure was subsequently devised. Categorization of foundational terms promotes concept understanding and improves literacy and application to genomics-based oncology practice. The ONS Genomics Taxonomy launched in August 2020 and can be accessed on the ONS Genomics and Precision Oncology Learning Library (www.ons.org/learning-libraries/precision-oncology). Consistent use of accurate terms using the ONS Genomics Taxonomy will be represented in all ONS materials. Adoption and standardization of the terms defined in the ONS Genomics Taxonomy will occur over time. The taxonomy consists of six categories with individual terms. Many terms include clinical scenarios and/or graphics. As the evidence base continues to evolve and expand, so will this taxonomy. Work has already begun on advanced genomic concepts that will be added to the taxonomy. Figure 1 depicts the categorization of the taxonomy as of March 2021.
Nursing Considerations
The ONS Genomics Taxonomy is relevant to oncology nursing because it directly affects oncology nursing practice. The field has moved from testing single genes to using multigene panel tests or even whole-genome sequencing. Indications for germline testing to identify inherited cancer risk are escalating (Lincoln et al., 2020). Pharmacogenomics is increasingly used to inform medication selection and optimal dosing and to identify contraindications. Gene expression analysis is part of evidence-based guidelines to predict recurrence risk to further inform adjuvant therapies in diseases such as breast cancer. Somatic (tumor) testing is also being used to inform targeted therapy selection. These applications represent just a few examples.
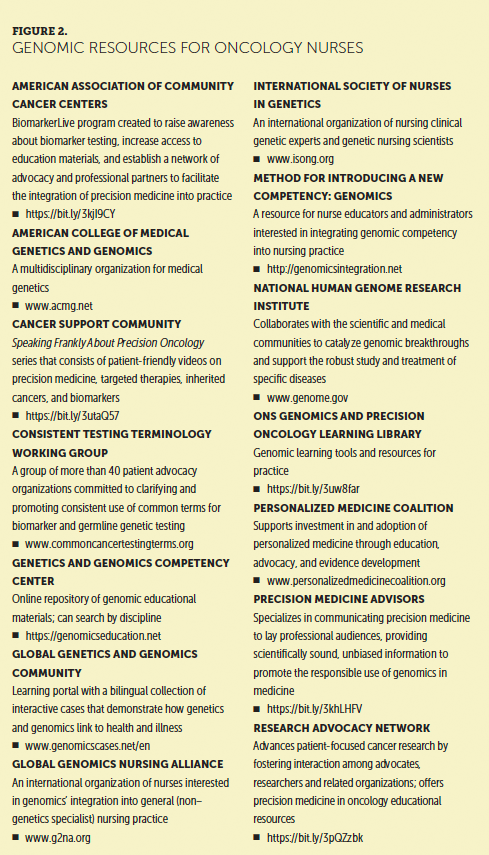
With this expansion of genomics in cancer care comes new terminology and the need to translate this information to the patient with cancer. For example, in the genomics era, terms such as “mutation” quickly became confusing and outdated. When testing capacity could be expanded to incorporate genes with varying levels of evidence and testing expanded to encompass inherited and tumor genomics, it became essential to standardize and classify genetic changes. As a result, new terminology and classification criteria were developed to help laboratories consistently classify the pathogenicity of the genetic change and communicate consistent information about what are now termed “variants” to healthcare providers (Richards et al., 2015). Additional nursing genomic resources are listed in Figure 2.
Conclusion
Misconceptions about foundational genomic concepts persist (Read & Ward, 2018), and oncology nurses cannot accurately apply genomic knowledge in practice unless they have genomic literacy. The ONS Genomics Taxonomy was developed to serve as a foundation for oncology nurses to be fluent in genomic terms, the underlying concepts, and their applications in practice. Use of this standard taxonomy enhances communication among healthcare providers and supports nurses when they educate patients and families about genomic concepts. This taxonomy will continue to reflect the current evidence and support oncology nurses integrating genomics into their practice, facilitating safe, quality patient care.
The authors gratefully acknowledge the Oncology Nursing Society Genomics Advisory Board members Elisabeth King, RN, FNP, AOCNP®, AGN, Suzanne M.Mahon, DNS, RN, AOCN®, AGN-BC, FAAN, Mary L. Schmitt, MS, APRN, FNP-BC, AOCNP®, and Kelliann C. Fee-Schroeder, BSN, RN, OCN®, for their review of the taxonomy.
About the Author(s)
Patricia Friend, PhD, APRN-CNS, AOCNS®, AGN-BC, is an associate professor and program director in the Marcella Niehoff School of Nursing at Loyola University Chicago in Illinois; Erin Dickman, MS, RN, OCN®, is an oncology clinical specialist at the Oncology Nursing Society in Pittsburgh, PA; and Kathleen Calzone, PhD, RN, AGN-BC, FAAN, is a research geneticist in the Genetics Branch of the Center for Cancer Research at the National Cancer Institute, National Institutes of Health, in Bethesda, MD. The authors take full responsibility for this content. This project received in-kind support from the Intramural Research Program of the National Institutes of Health, National Cancer Institute. Friend can be reached at pfriend@luc.edu, with copy to CJONEditor@ons.org.
References
Aiello, L.B. (2017). Genomics education: Knowledge of nurses across the profession and integration into practice. Clinical Journal of Oncology Nursing, 21(6), 747–753. https://doi.org/10.1188/17.CJON.747-753
Bever, L. (2017, October 24). ‘Damaged for the rest of my life’: Woman says surgeons mistakenly removed her breasts and uterus. Washington Post. https://www.washingtonpost.com/news/to-your-health/wp/2017/10/24/damage…
Bonadies, D.C., Brierley, K.L., Barnett, R.E., Baxter, M.D., Donenberg, T., Ducaine, W.L., . . . Matloff, E.T. (2014). Adverse events in cancer genetic testing: The third case series. Cancer Journal, 20(4), 246–253. https://doi.org/10.1097/PPO.0000000000000057
Brierley, K.L., Blouch, E., Cogswell, W., Homer, J.P., Pencarinha, D., Stanislaw, C.L., & Matloff, E.T. (2012). Adverse events in cancer genetic testing: Medical, ethical, legal, and financial implications. Cancer Journal, 18(4), 303–309. https://doi.org/10.1097/PPO.0b013e3182609490
Farmer, M.B., Bonadies, D.C., Mahon, S.M., Baker, M.J., Ghate, S.M., Munro, C., . . . Matloff, E.T. (2019). Adverse events in genetic testing: The fourth case series. Cancer Journal, 25(4), 231–236. https://doi.org/10.1097/PPO.0000000000000391
Giri, V.N., Knudsen, K.E., Kelly, W.K., Cheng, H.H., Cooney, K.A., Cookson, M.S., . . . Gomella, L.G. (2020). Implementation of germline testing for prostate cancer: Philadelphia Prostate Cancer Consensus Conference 2019. Journal of Clinical Oncology, 38(24), 2798–2811. https://doi.org/10.1200/JCO.20.00046
Haga, S.B., Mills, R., & Bosworth, H. (2014). Striking a balance in communicating pharmacogenetic test results: Promoting comprehension and minimizing adverse psychological and behavioral response. Patient Education and Counseling, 97(1), 10-15. https://doi.org/10.1016/j.pec.2014.06.007
Kohn, L.T. (2001). The Institute of Medicine report on medical error: Overview and implications for pharmacy. American Journal of Health-System Pharmacy, 58(1), 63-66. https://doi.org/10.1093/ajhp/58.1.63
Lincoln, S.E., Nussbaum, R.L., Kurian, A.W., Nielsen, S.M., Das, K., Michalski, S., . . . Esplin, E.D. (2020). Yield and utility of germline testing following tumor sequencing in patients with cancer. JAMA Network Open, 3(10), e2019452. https://doi.org/10.1001/jamanetworkopen.2020.19452
Macklin, S.K., Jackson, J.L., Atwal, P.S., & Hines, S.L. (2019). Physician interpretation of variants of uncertain significance. Familial Cancer, 18(1), 121–126. https://doi.org/10.1007/s10689-018-0086-2
Mahon, S.M. (2019). Coordination of genetic care: More important and complicated than it seems. Journal of the National Comprehensive Cancer Network, 17(11), 1272–1276. https://doi.org/10.6004/jnccn.2019.7343
Martin, N.A., Friedman, S.J., Saxton, C., Yarden, R., Lindsey, S., Kuhn, E., . . . Horn, M.K. (2020). Using consistent terms in precision medicine to eliminate patient confusion. Journal of Clinical Oncology, 38(15, Suppl.), e24164–e24164. https://doi.org/10.1200/JCO.2020.38.15_suppl.e24164
National Human Genome Research Institute. (2020a, December 7). DNA sequencing costs: Data. https://www.genome.gov/about-genomics/fact-sheets/DNA-Sequencing-Costs-…
National Human Genome Research Institute. (2020b). Talking glossary of genetic terms. https://www.genome.gov/genetics-glossary/c#glossary
Ray, T. (2017, October 27). Oregon lawsuit highlights importance of genetic counseling during period of increasing test access. https://www.genomeweb.com/cancer/oregon-lawsuit-highlights-importance-g…
Read, C.Y., & Ward, L.D. (2018). Misconceptions about genomics among nursing faculty and students. Nurse Educator, 43(4), 196-200. https://doi.org/10.1097/NNE.0000000000000444
Richards, S., Aziz, N., Bale, S., Bick, D., Das, S., Gastier-Foster, J., . . . Rehm, H.L. (2015). Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genetic Medicine, 17(5), 405-423. https://doi.org/10.1038/gim.2015.30


