Radiodermatitis in Patients With Cancer: Systematic Review and Meta-Analysis
Problem Identification: A systematic review and meta-analysis was conducted to inform the development of guidelines on the management of radiodermatitis among patients with cancer.
Literature Search: The authors updated a systematic review to include available literature published through September 30, 2019.
Data Evaluation: Two investigators assessed risk of bias using the Cochrane Collaboration risk-of-bias tool and certainty of the evidence using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach.
Synthesis: The use of deodorant/antiperspirant had no effect on development of radiodermatitis. Aloe vera and emu oil were equivalent or less effective than standard care. Oral curcumin had a minimal beneficial effect. Nonsteroidal topical interventions had a minimal beneficial effect on the development of moist desquamation and relief of itching while causing a small increase for grade 2 radiodermatitis. Topical calendula increased risk for the development of radiodermatitis. Topical steroids and dressings each showed benefits to minimize the development of radiodermatitis and moist desquamation while lowering rates of patient-reported symptoms, such as pain and pruritus.
Implications for Research: Symptom management strategies for radiodermatitis among patients with cancer that are likely to be effective include topical nonsteroidals, topical steroids, and dressings.
Supplemental material can be found at https://bit.ly/2FWj3Kp
Jump to a section
Radiation therapy is one of the pillars of cancer treatment that has led to an increase in cancer survival rates in the United States. In 2000, about 24% of cancer survivors received radiation and, in 2020, that number was expected to increase to 29% (Bryant et al., 2017). This increase was seen across cancer sites, with the largest increases for patients being treated for breast or prostate cancer (Bryant et al., 2017). A prevalent side effect of ionizing radiation is radiodermatitis (also referred to as radiation dermatitis or radiation-induced skin reaction). An estimated 95% of patients who receive radiation therapy will develop some level of radiodermatitis (Singh et al., 2016). Because of this high risk, interventions for radiodermatitis are aimed at minimizing the severity or delaying progression to higher grades, rather than prevention.
Skin changes from radiation therapy are caused by disruption to the normal process of cell division and repair related to ionizing radiation therapy (Bray et al., 2016). Radiodermatitis can range from mild erythema to dry desquamation and moist desquamation (Singh et al., 2016). These skin changes usually manifest within two to three weeks of radiation initiation and can persist for as long as four weeks following the completion of treatment (Naylor & Mallett, 2001). Radiodermatitis can be painful and uncomfortable to patients and can have a negative effect on quality of life (Aistars, 2006; Vaz et al., 2007). If severe, it can also lead to changes in radiation treatment schedules (McQuestion, 2006).
Various products have been studied in the literature to minimize radiodermatitis with limited consensus to support a standard of care. Variation in products studied and research methodologies employed have led to inconsistency in practice recommendations, even within the same institution (Bieck & Phillips, 2010; Feight et al., 2011). An evidence-based review of available studies found insufficient evidence to support interventions, other than basic skin care hygiene (washing the irradiated skin with mild soap and water) (Feight et al., 2011).
Although no gold standard exists for the management of radiodermatitis, research is emerging and methodologies are available to synthesize the evidence to build clinical guidelines that inform decisions at the point of care. The goal of this review is to update the research evidence and serve as the foundation for a practice guideline on interventions for the management of radiodermatitis for patients with cancer.
This systematic review accompanies and informs the evidence base for the Oncology Nursing Society (ONS) Guidelines™ on the management of radiodermatitis in patients with cancer. This review presents the comparative efficacy of eight interventions to minimize the development of radiodermatitis and to treat radiodermatitis in patients with cancer.
Methods
This systematic review was conducted in three stages: (a) published systematic reviews matching the PICO (population, intervention, comparator, outcomes) questions were reviewed and appraised with the AMSTAR 2 (A Measurement Tool to Assess Systematic Reviews–2) criteria (Shea et al., 2017) to determine if any met sufficient quality to inform the guidelines; (b) for reviews meeting these criteria, an updated literature search was performed; and (c) for questions for which there was either not a published systematic review of sufficient quality or no relevant published systematic review, a de novo systematic review was conducted. The systematic review protocol was registered with PROSPERO (CRD42019135778) and was guided by the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) reporting process.
PICO Questions
This review was guided by the PICO format, which frames clinical questions with the following components: defining a specific patient population, intervention, comparator, and outcomes. The questions were identified by a group of clinical experts (nurses, radiation oncologists, patient representative). This group was tasked with identifying timely, relevant questions that patients with cancer have regarding radiodermatitis and questions about which clinicians have uncertainty. For each question, the clinical experts selected patient-important questions a priori. The questions focused on patients with cancer receiving radiation therapy and interventions to minimize or treat radiodermatitis during cancer treatment. A full list of the PICO questions is included in the Appendix.
Search Strategy and Inclusion Criteria
At the outset, several published systematic reviews that closely addressed the PICO questions were reviewed by team members using the AMSTAR 2 approach. One review was determined to be of sufficient quality to inform the PICO questions. For the current systematic review, a medial librarian replicated the MEDLINE®, EMBASE®, CINAHL®, Wiley Cochrane Library, PsycINFO®, and LILACS search strategies previously published (Chan, Webster, et al., 2014) to update the literature search through September 2019. The primary outcomes were classified as development of radiodermatitis, pain, pruritus, quality of life, adverse events, and intervention adherence and fidelity. The full search strategies and critical outcomes are presented in the Appendix.
Any grey literature (such as conference abstracts) retrieved in any of the database searches was excluded unless the study results or data were subsequently published in a peer-reviewed journal. All citation results from the searches were imported into Covidence® software. Two reviewers independently screened all citation titles and abstracts based on inclusion and exclusion criteria. Inclusion criteria were randomized controlled trials (RCTs), nonrandomized study with a comparison group, management or treatment of radiodermatitis, and adult population. Exclusion criteria were non-English studies, studies without a control group, pediatrics, and systematic reviews. Citations that were approved by two reviewers proceeded to full-text screening, with any conflicts resolved by the team leader.
Data Extraction
Two investigators, independently and in duplicate, extracted all data into a pilot-tested Microsoft Excel® spreadsheet. Any discrepancies or errors were resolved after consulting with the original source and consensus among two investigators. If consensus could not be reached, then a decision was made with consultation from the team leader or methodologist. Outcome data were entered into Review Manager® (RevMan) software.
Data Synthesis and Analysis
When possible, outcome data for each comparison were analyzed quantitatively by calculating a pooled effect in RevMan. The pooled analysis was presented as a risk ratio (RR) for dichotomous variables and either a mean difference (MD) or standard MD for continuous variables. RevMan uses the DerSimonian and Laird (1986) method for random- and fixed-effects models to determine the overall effect size, with 95% confidence intervals (CIs). In situations for which quantitative data could not be pooled, the outcomes were expressed narratively.
Risk of Bias and Assessing the Certainty of the Evidence
The Cochrane Collaboration risk-of-bias tool was used to assess individual study bias for RCTs (Higgins et al., 2011). Domains reported in this tool include sequence generation, allocation concealment, blinding of participants, personnel and outcome assessors, incomplete outcome data, selective reporting, and other sources of bias. Each domain was rated to be at low, high, or unclear risk of bias. Two reviewers independently assessed risk of bias for included studies with disagreements resolved by discussion and consensus with another investigator (see Appendix).
The overall certainty of evidence was assessed using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach (Guyatt et al., 2011). The certainty in the estimate of effects across the body of evidence for each outcome was rated according to the following domains: study limitations (risk of bias), inconsistency (heterogeneity), indirectness, imprecision, and publication bias. The overall certainty of evidence across all outcomes was classified as high, moderate, low, or very low. The graded evidence across outcomes for each comparison is presented in a summary of findings table, generated from the GRADEpro GDT, in the Appendix.
Results
Search results are illustrated in a PRISMA diagram (see Figure 1). In total, the authors identified 4,376 citations from the electronic databases. Four articles were identified through hand searching. After removal of duplicates and screening titles and abstracts, 94 articles were available for full-text review. Of these 94 titles, the authors included 22 titles (23 studies) involving 3,127 participants and excluded 72 that did not meet the selection criteria (see Tables 1 and 2). 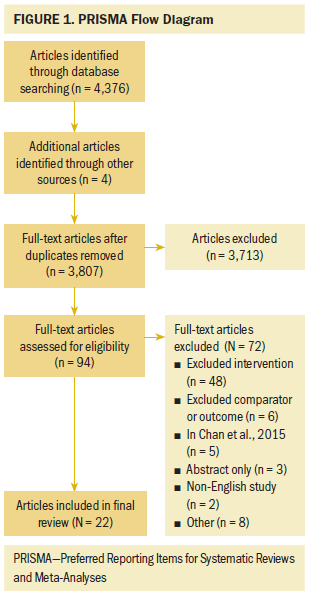
Data Synthesis
Should deodorant/antiperspirant in addition to normal washing be used rather than normal washing alone in patients receiving radiation therapy for cancer in the breast/chest region?
The systematic review identified five studies that addressed this question, all in patients with breast cancer (Bennett, 2009; Gee et al., 2000; Lewis et al., 2014; Théberge et al., 2009; Watson et al., 2012). Sample sizes ranged from 36 to 333. Lewis et al. (2014) compared aluminum-containing deodorant to non–aluminum-containing deodorant to soap, and the other four studies compared deodorant or antiperspirant to a control group of no deodorant or antiperspirant. The analysis reviewed aluminum- and non–aluminum-containing deodorant data as compared with soap separately and found the odds of sweating reduced among the aluminum-containing deodorant and non–aluminum-containing deodorant groups (odds ratio [OR] = 0.15, 95% CI [0.03, 0.91] and OR = 0.61, 95% CI [0.17, 2.19], respectively); however, no difference was noted for the outcomes of RTOG skin toxicity, axillary pain, itch, and burning. 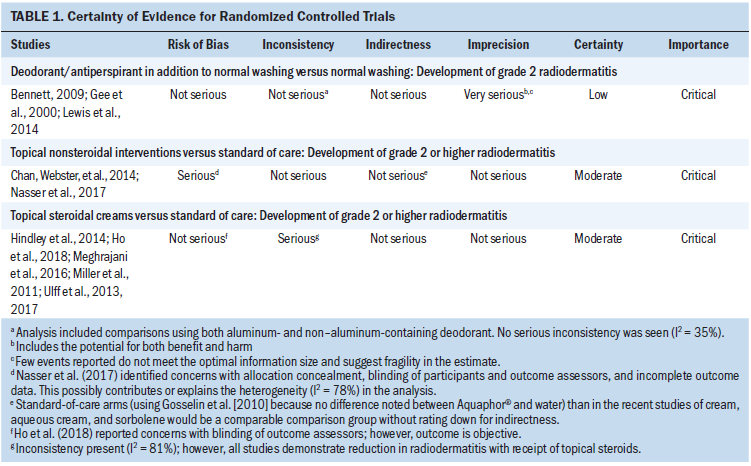
When comparing the evidence for use of any deodorant or antiperspirant, the use of deodorant or antiperspirant had no effect on the development of grade 2 radiodermatitis (RR = 0.99, 95% CI [0.76, 1.29]; absolute risk reduction [ARR] 3 fewer per 1,000, from 84 fewer to 101 more; low certainty of evidence) (see Table 3) and minimal effect on development of grade 3 radiodermatitis (RR = 0.74, 95% CI [0.27, 2.02]; ARR 13 fewer per 1,000, from 37 fewer to 52 more; low certainty of evidence). The study by Théberge et al. (2009) assessed patient reported outcomes at two weeks follow-up and identified no statistically significant differences in grade 2 axillary or breast radiodermatitis, axillary moist desquamation, general discomfort, pain, pruritus, or sweating. 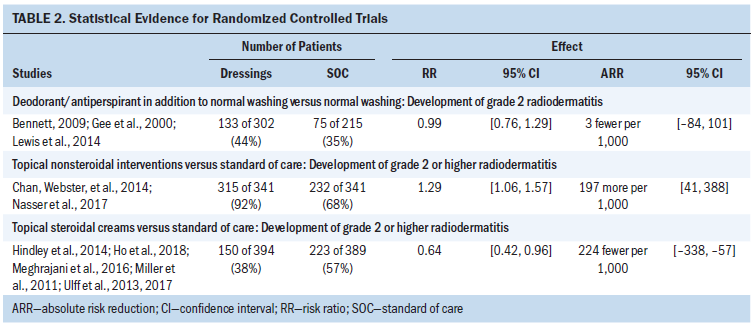
Should aloe vera lotion rather than standard of care be used to minimize the development of radiodermatitis?
This question was informed by four studies in the original systematic review (Heggie et al., 2002; Merchant et al., 2007; Olsen et al., 2001; Williams et al., 1996) and two added studies (Haddad et al., 2013; Hoopfer et al., 2015). Because of the heterogeneity of interventions included, the results could not be pooled. Sample sizes ranged from 60 to 248 and included studies of patients with breast cancer or samples with mixed cancer diagnoses. Aloe vera was compared to a placebo, soap, no treatment, and anionic phospholipid cream. Formulations included aloe vera gel, a commercially available product that includes aloe vera, and an aloe cream prepared specifically for the study. 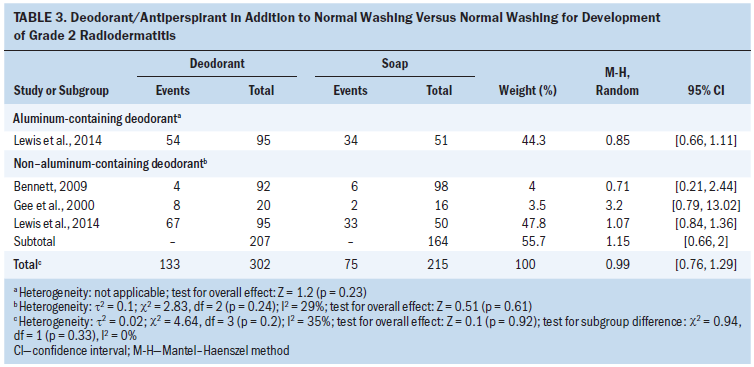
Aloe was found to be equivalent or less effective than the control in reducing grade or time to development of radiation dermatitis or of symptoms associated with radiation dermatitis, such as pain (Heggie et al., 2002; Hoopfer et al., 2015; Merchant et al., 2007; Williams et al., 1996). The study by Olsen et al. (2001) compared aloe gel to mild soap and found that, as the cumulative dose of radiation increased (more than 2,700 cGy), a protective effect was seen by adding aloe to the soap regimen. Haddad et al. (2013) reported that prophylactic use of aloe vera reduced the intensity of radiation dermatitis at week 4 during radiation therapy and at week 4 after radiation therapy (mean grade of dermatitis with and without aloe vera was 0.81 and 1.1 [p < 0.001] and 0.05 and 0.21 [p = 0.002], respectively).
Should emu oil rather than standard of care be used to minimize the development of radiodermatitis?
This question was informed by one study (Rollman et al., 2015). This was a single-institution feasibility and safety study of emu oil on skin-related toxicity for patients receiving radiation therapy to the breast or chest wall. Forty-five patients with breast cancer were randomized to emu oil or a placebo of cottonseed oil.
In this study, peak toxicity (as measured by the Common Terminology Criteria for Adverse Events) (National Cancer Institute, 2017) was seen at six weeks, and patients in the emu oil group had minimally worse toxicity grades, but the results were not statistically significant; however, the raw data was not reported. Patient-reported outcomes (Skindex scores for symptoms, emotional, and functional) trended lower in patients in the emu oil group than in the placebo group (mean total area under the curve = 7.2 versus 10.4, respectively; p = 0.29). Overall quality of life was minimally better for patients in the emu oil group, but remained stable throughout the study for both groups (Rollman et al., 2015).
Should oral curcumin rather than standard of care be used to minimize the development of radiodermatitis?
This question was informed by two studies (Ryan et al., 2013; Ryan Wolf et al., 2018) that investigated oral curcumin (6 g daily) during radiation therapy in patients with breast cancer. The sample size was 30 in the initial study and 686 in the follow-up study. Patients took four 500 mg capsules or placebo three times a day throughout radiation treatment (Ryan et al., 2013) and for an additional week after treatment (Ryan Wolf et al., 2018).
Oral curcumin may reduce the development of grade 2 or higher radiodermatitis (RR = 0.64, 95% CI [0.42, 0.96]; ARR = 48 fewer per 1,000, from 78 fewer to 5 fewer; very low certainty of evidence) and radiodermatitis at end of treatment (MD = 0.8 lower, from 1.36 lower to 0.23 lower; very low certainty of evidence).
Should topical nonsteroidal interventions (creams, lotions, ointments) rather than standard of care be used for the minimization or treatment of radiodermatitis?
The authors identified three RCTs that addressed this question (Chan, Mann, et al., 2014; Laffin et al., 2015; Nasser et al., 2017). Additional studies were identified that included a variety of interventions and comparators. Based on findings from Gosselin et al. (2010), which demonstrated no difference between the effect of Aquaphor® and water, the review panel considered aqueous cream (e.g., Aquaphor, sorbelene) as the standard of care. Therefore, the review panel excluded studies that compared an intervention to an active comparator or did not report outcomes of radiodermatitis. Sample sizes for included studies ranged from 23 to 255, with two studies of patients with breast cancer and one of patients with breast, lung, or head and neck cancer. The topical nonsteroidal treatments used in the studies included vitamin D ointment, Cavilon™ barrier cream, and an oil-based emulsion containing allantoin. Comparison groups received an aqueous or moisturizing cream.
The use of topical nonsteroidal interventions resulted in a small increase in risk of the development of grade 2 or higher radiodermatitis (RR = 1.29, 95% CI [1.06, 1.57]; ARR = 197 more per 1,000, from 41 more to 388 more; moderate certainty of evidence) (see Table 4). A small decrease in development of moist desquamation (RR = 0.84, 95% CI [0.46, 1.56]; ARR = 26 fewer per 1,000, from 86 fewer to 90 more; very low certainty of evidence) and relief of itching were noted (RR = 0.85, 95% CI [0.73, 0.99]; ARR = 127 fewer per 1,000, from 229 fewer to 8 fewer; very low certainty of evidence). Minimal effect was noted in the symptoms of pruritis (RR = 1.09, 95% CI [0.95, 1.24]; ARR = 35 more per 1,000; from 19 fewer to 93 more, low certainty of evidence) and pain (RR = 1.1, 95% CI [0.9, 1.35]; ARR = 35 more per 1,000, from 35 fewer to 122 more; moderate certainty of evidence). 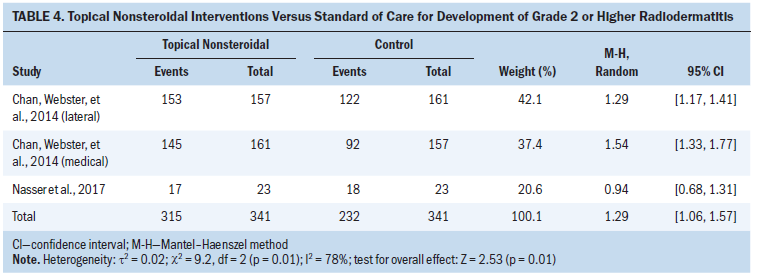
Should calendula rather than standard of care be used to minimize the development of radiodermatitis?
The evidence for this question was informed by two studies (Schneider et al., 2015; Sharp et al., 2013). Schneider et al. (2015) conducted an RCT that included 51 patients with cancer of the head and neck and compared calendula to essential fatty acids (the standard of care at the institution where the research was conducted). Sharp et al. (2013) compared calendula to Essex (a moisturizing cream) in 420 patients with a variety of cancer diagnoses. A third study by Pommier et al. (2004) was identified but was excluded from analysis because of the use of trolamine in the control group.
Sharp et al. (2013) reported no differences between the groups in the patient-reported symptoms of pain, burning, itching, pulling, or tenderness during the duration of the study, but did report that incidence of grade 2 or higher skin reaction was 23% in the calendula group and 19% in the Essex group at follow-up (5–17 days after final radiation treatment). In addition, Sharp et al. (2013) did not find a statistically significant difference between calendula and Essex in health-related quality of life or sleeping patterns at follow-up. Patients favored Essex for application (p < 0.001) and absorption (p < 0.001), with no differences in scent of product or adherence to product during the study (Sharp et al., 2013). The study by Schneider et al. (2015) did not include patient-reported or quality-of-life outcomes. The authors reported grade 2 skin reaction in 35% of patients who received essential fatty acids and grade 2 and 3 skin reaction in 14% of patients in the calendula group at the 25th radiation treatment session (Schneider et al., 2015). The use of calendula during radiation therapy may increase the risk of developing grade 2 or higher radiodermatitis (RR = 1.21, 95% CI [0.83, 1.77]; ARR = 36 more per 1,000, from 29 fewer to 131 more; low certainty of evidence).
Should topical steroidal creams rather than standard of care be used for the minimization or treatment of radiodermatitis?
The evidence for this question was informed by six RCTs (Hindley et al., 2014; Ho et al., 2018; Meghrahani et al., 2016; Miller et al., 2011; Ulff et al., 2013, 2017) all in patients with breast cancer. Sample sizes ranged from 50 to 202. Topical steroid creams included betamethasone (2), mometasone (2), and hydrocortisone (1), with comparisons including moisturizing creams (4) or diprobase (1).
Topical steroidal creams moderately reduced the development of grade 2 or higher radiodermatitis (RR = 0.64, 95% CI [0.42, 0.96]; ARR = 224 fewer per 1,000, from 338 fewer to 57 fewer; moderate certainty of evidence) (see Table 5) and moist desquamation (RR = 0.57, 95% CI [0.29, 1.12]; ARR = 161 fewer per 1,000, from 266 fewer to 45 more; low certainty of evidence). Topical steroids strongly reduced pain (measured by severe visual acuity scale of itching, burning, and irritation) during radiation treatment (RR = 0.12, 95% CI [0.02, 0.98]; ARR = 62 fewer per 1,000, from 69 fewer to 1 fewer; low certainty of evidence) and pain after radiation treatment (RR = 0.05, 95% CI [0.01, 0.39]; ARR = 178 fewer per 1,000, from 186 fewer to 114 fewer; moderate certainty of evidence). Treatment-related adverse events may be higher in patients who received topical steroids (RR = 2.35, 95% CI [0.23, 24.26]; ARR = 50 more per 1,000, from 29 fewer to 861 more; low certainty of evidence). 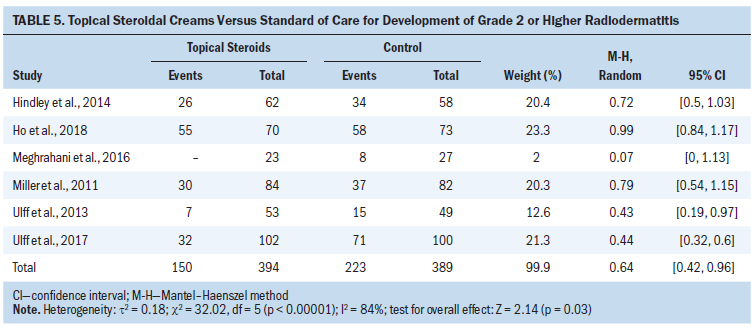
Should semipermeable dressings rather than standard of care be used for the minimization or treatment of radiodermatitis?
The evidence for this question was informed by eight RCTs (Chan et al., 2019; Herst et al., 2014; Lam et al., 2019; MØller et al., 2018; Rades et al., 2019; Schmeel et al., 2018; Wooding et al., 2018; Zhong et al., 2013). Sample sizes ranged from 36 to 197, and interventions included Mepitel® film, StrataXRT®, hydrofilm, 3M™ Cavilon™ barrier film, and Mepilex® Lite. Comparisons were sorbolene, aqueous cream, and standard of care (including saline wash). Patient populations included patients with breast cancer or head and neck cancer. All but one study included application of semipermeable dressings from the start of radiation therapy.
Semipermeable dressings had a moderate protective effect on the development of grade 2 or higher radiodermatitis (RR = 0.52, 95% CI [0.26, 1.03]; ARR = 224 fewer per 1,000, from 346 fewer to 14 more; low certainty of evidence) and on the development of moist desquamation (RR = 0.43, 95% CI [0.32, 0.58]; ARR = 205 fewer per 1,000, from 244 fewer to 151 fewer; low certainty of evidence). Patient-reported symptoms were also minimized by dressings in the included studies. A large protective effect for dressings was found for tenderness, discomfort, or pain (RR = 0.35, 95% CI [0.16, 0.78]; ARR = 167 fewer per 1,000, from 215 fewer to 56 fewer; low certainty of evidence), and a moderate effect was seen for pruritus (RR = 0.69, 95% CI [0.34, 1.38]; ARR = 64 fewer per 1,000, from 137 fewer to 79 more; very low certainty of evidence). A beneficial effect was seen in quality of life (MD = 0.4 lower, from 0.75 lower to 0.05 lower; very low certainty of evidence), but the clinical significance of this is likely small. Twenty-one percent of patients (19 of 90) receiving dressing experienced adverse events leading to treatment discontinuation. Although there are some concerns with fragility related to the few events reported (only in the treatment arm), patients using dressing experienced more adverse events than those not using dressings (RR = 20.4, 95% CI [2.82, 147.52]; moderate certainty of evidence).
Only one study reported on treatment with semipermeable dressings as compared with a control arm treated with salt water among patients with head and neck cancer after radiodermatitis had presented. For patients with radiodermatitis, semipermeable dressings may reduce the number of days until resolution of radiodermatitis as compared to salt water (MD = –7 days; 95% CI [–11.86, –2.14]; low certainty of evidence).
Discussion
Statement of the Principle Findings
This article aimed to synthesize the research findings on interventions to minimize and treat radiodermatitis in patients with cancer. The authors updated a thorough and high-quality systematic review conducted by Chan, Webster, et al. (2014) and expanded on it to include additional interventions. The use of deodorant or antiperspirant and topical use of aloe vera or emu oil had no effect on the development of radiodermatitis. Oral curcumin had a minimal positive effect in two studies. The use of topical calendula increased risk of radiodermatitis. Topical nonsteroidal interventions to minimize the development of radiodermatitis had small benefits for moist desquamation and relief of itching, but had a small increase in the development of grade 2 or higher radiodermatitis. Topical steroids and dressings each had beneficial effects on the development of radiodermatitis and moist desquamation, as well as patient-reported symptoms, but also showed an increase in adverse events.
Strengths and Limitations
Although the body of evidence comparing interventions for the management of radiodermatitis was limited, the authors used a rigorous and transparent methodology for the identification of eligible studies, meta-analysis, and grading of the evidence. Both randomized and nonrandomized comparison studies were eligible for inclusion in the analysis. Although the initial search may have identified grey literature, the authors only included published, peer-reviewed studies in the analysis. The authors only included English-language publications, and it is possible that some relevant non-English literature may have been missed.
Relation to Other Studies
Systematic reviews of the research on management of radiodermatitis are available and offer guidance to future research and clinical care. A review by Rosenthal et al. (2019) included topical agents that have been studied for acute radiation dermatitis. In this narrative review, they report that basic washing practice with mild soap and water are recommended as standard of care. For herbal options, they report that aloe vera has not been shown to reduce severe radiodermatitis and that calendula significantly lowered the frequency of grade 2 or higher dermatitis. They also reported benefits with topical steroids and dressings, but no meta-analysis was included. A review that focused on patients with breast cancer reported that few topical agents and oral supplements were effective across RCTs reviewed, but that newer radiotherapy techniques consistently demonstrated a decrease in rates of radiodermatitis (Yee et al., 2018). The current review builds on these findings by systematically gathering data from available literature and identifying potential areas of promise in radiodermatitis treatment and areas in need of future research.
Nursing Considerations
Radiodermatitis remains a frequent adverse effect of treatment with radiation therapy (Ho et al., 2018; Salvo et al., 2010). Advances in radiation therapy techniques have improved patient outcomes; however, skin changes from treatment remain prevalent, with a majority of patients experiencing dry desquamation (85% in a sample of mixed cancer types) or moist desquamation (15%) that requires wound dressing (Chan, Mann, et al., 2014). Despite the prominence of this adverse effect and a growing body of research, guidance for best practice in the management of radiodermatitis is still evolving. An editorial by Chan (2019) included several thoughtful recommendations for future work in this area. The first recommendation is to undertake a systematic review to identify gaps to understand why previous studies were not effective and which areas of research hold promise. Second, understanding relevant mechanisms of action will be important to plan future interventions. Lastly, patient burden should be considered, and only the most promising interventions should be studied (Chan, 2019). After completing the current review of available literature, the authors concur with these recommendations and add that standard outcome measurements, such as quality of life and related symptoms (e.g., pain), be included in future research, as well as standard time frames for assessment to allow for comparison across studies. Nurses have a pivotal role in the care and management of patients during and after radiation treatment and can lead evidence-based practice and quality improvement projects that incorporate best evidence into patient care.
Conclusion
The research included in this systematic review provides low to moderate evidence on interventions to minimize the development of radiodermatitis and for treatment when it occurs. The evidence in this review also informs an accompanying clinical practice guideline (Gosselin et al., 2020) on the management of radiodermatitis in patients with cancer to enable nurses and other healthcare providers in the implementation of evidence-based interventions for radiodermatitis in clinical settings.
About the Author(s)
Pamela K. Ginex, EdD, RN, OCN®, is the senior manager of evidence-based practice and inquiry, and Chelsea Backler, MSN, APRN, AGCNS-BC, AOCNS®, is an oncology clinical specialist, both at the Oncology Nursing Society in Pittsburgh, PA; Elizabeth Croson, PhD, RN, MSN, is a course instructor at Western Governor’s University in Salt Lake City, UT; Lindsey N. Horrell, PhD, MPH, RN, is a postdoctoral fellow in the Gillings School of Global Public Health at the University of North Carolina at Chapel Hill; Kerri A. Moriarty, MLS, is a research specialist and, at the time of this writing, Christine Maloney, BA, was an archivist and Mark Vrabel, MLS, AHIP, ELS, was an information resources supervisor, all at the Oncology Nursing Society; and Rebecca L. Morgan, PhD, MPH, is an assistant professor in the Department of Health Research Methods, Evidence, and Impact at McMaster University in Hamilton, Ontario, Canada. Development of this review was wholly funded by the Oncology Nursing Society, a nonprofit organization that represents oncology nurses. No honoraria were provided. Mention of specific products and opinions related to those products do not indicate or imply endorsement by the Oncology Nursing Society. Ginex, Backler, and Morgan contributed to the conceptualization and design and provided statistical support. All authors completed the data collection. Ginex, Backler, Croson, and Morgan provided analysis. Ginex, Backler, Horrell, and Morgan contributed to the manuscript preparation. Ginex can be reached at pginex@ons.org, with copy to ONFEditor@ons.org. (Submitted May 2020. Accepted July 20, 2020.)


