Symptoms and Health-Related Quality of Life in Patients Receiving Cancer Therapy Matched to Genomic Profiles
Objectives: To examine symptom occurrence and severity and overall health-related quality of life (HRQOL) in patients receiving cancer therapy guided by genomic profiling (matched therapy) and patients receiving nonmatched therapy.
Sample & Setting: A retrospective and secondary analysis of data from 129 individuals with breast or gynecologic cancer receiving care at a regional outpatient cancer center.
Methods & Variables: Descriptive statistics and multiple linear regression analyses were performed. Study variables included symptom occurrence and severity, HRQOL, and person- and health-/illness-related factors. Symptom occurrence and severity were measured by the Therapy-Related Symptom Checklist (TRSC), and HRQOL was measured by the HRQOL–Linear Analogue Self-Assessment.
Results: Individuals receiving matched therapy had lower mean TRSC scores compared to individuals receiving nonmatched therapy, but the difference was not statistically significant. HRQOL scores among individuals receiving matched therapy were not significantly higher than those receiving nonmatched therapy. Individuals with higher TRSC scores had significantly lower HRQOL.
Implications for Nursing: The effects of matched therapy on an individual should be examined. Study findings are an initial step in understanding the symptom occurrence and severity and HRQOL.
Jump to a section
Breast and gynecologic cancers comprise more than 375,000 of new cancer cases annually (American Cancer Society, 2018). Although advancements in screening and treatment have reduced death rates, a significant proportion of women will require long-term treatment for their cancer. Many physical and emotional symptoms are experienced throughout the cancer continuum, negatively affecting health-related quality of life (HRQOL) (Huang et al., 2017; Miaskowski et al., 2017). Identification of these symptoms is essential because their management can enhance HRQOL and lead to greater adherence to treatment and, therefore, improved efficacy (Smith, Sestak, Howell, Forbes, & Cuzick, 2017).
State-of-the-art cancer care includes personalizing strategies to treat an individual’s cancer based on his or her unique genomic signature found by genomic profiling. Genomic profiling identifies the tumor-specific alterations in DNA and molecular pathways that can influence the development and progression of cancer and is increasingly being incorporated into routine clinical practice so that the therapies selected are more precise. Cancer treatment based on genomic profiling has been referred to as matched therapy (Schwaederle et al., 2016; Tsimberidou et al., 2012, 2014). Matched therapy is part of the broader precision medicine initiative, which considers individual variability in genes, environment, and lifestyle to customize the treatment for each person. The use of precision medicine is most advanced in the treatment of cancer (U.S. Food and Drug Administration, 2017). Matched therapy often includes the use of targeted therapies, which are drugs that block the growth and/or spread of cancer by interfering with specific molecules involved in the growth and/or spread of cancer (National Cancer Institute, 2018). Targeted therapies have unique side effect profiles compared to chemotherapy, including dermatologic, endocrine, vascular, immunologic, and pulmonary toxicities (Dy & Adjei, 2013).
An important issue to consider is the tolerability of matched therapy because it often involves combining drugs in a novel way that is based on an individual’s unique genomic profile, and these individuals may have narrow therapeutic windows (Nikanjam, Liu, & Kurzrock, 2016). Novel drug combinations that are matched to genomic profile results have shown beneficial outcomes and are increasingly being used (Schwaederle et al., 2015, 2016). Although matched therapy brings the hope of increased efficacy, little is known about the symptom experience or HRQOL for individuals undergoing this therapy. Prior studies examining symptoms and HRQOL related to cancer treatment have focused on nonmatched therapy (e.g., chemotherapy, radiation) (Kirkova, Aktas, Walsh, & Davis, 2011; Reeve et al., 2014). In addition, clinical trials of contemporary therapies, such as targeted therapies, rely on clinician-reported toxicities versus patient-reported symptom assessments (Kluetz, Chingos, Basch, & Mitchell, 2016). A study to examine the symptoms experienced by individuals receiving matched therapy and potential influence on HRQOL is considered to be a valuable endeavor given the current gaps in knowledge. Understanding the impact on individuals receiving this increasingly used approach for cancer treatment will be an important first step in the eventual goal of preventing, identifying, and treating these symptoms, which can cause suffering and distress (Cleeland, 2000; Kirkova et al., 2010) and reduce HRQOL (Janz et al., 2007; Miaskowski et al., 2006). The objectives of this study were as follows:
• To describe the characteristics of individuals receiving matched and nonmatched therapies for cancer
• To describe and compare symptom occurrence and severity and HRQOL by therapy type (matched versus nonmatched)
• To examine the association between therapy type and overall symptom occurrence and severity, as reported on the Therapy-Related Symptom Checklist (TRSC), after controlling for person- and health-/illness-related factors
• To examine the relationship between therapy type and HRQOL, as reported on the HRQOL–Linear Analogue Self-Assessment (HRQOL-LASA), after controlling for person- and health-/illness-related factors and symptom occurrence and severity.
Variables of interest were guided by a review of the literature and relevant concepts within the symptom management theory (Dodd et al., 2001).
Methods
This study had a retrospective, correlational design with a secondary analysis of data from individuals with breast or gynecologic cancer who were enrolled in one of two parent studies conducted from August 2014 to September 2016 at Avera Cancer Institute in Sioux Falls, South Dakota. One study evaluated the effects of co-administration of metformin and doxorubicin during neoadjuvant or adjuvant treatment for breast cancer on left ventricle ejection fraction (NCT02472353). In this study, a convenience sample of 30 participants consented and were randomized to receive metformin or no metformin. All participants received neoadjuvant or adjuvant doxorubicin for breast cancer treatment; data from 27 participants were available for this study. Remaining data were from a convenience sample of participants with cancer who consented and were enrolled to a study that identified tumor-specific alterations by performing cancer genomic profiling (NCT02470715). If applicable, genomic profile results were used to suggest a matched treatment. All matched treatments involved U.S. Food and Drug Administration–approved therapies; however, the therapies may have been for off-label use and involved novel combinations in some cases. In both studies, symptom occurrence and severity and HRQOL were measured with the TRSC and HRQOL-LASA, respectively.
The sample for this study included women who were enrolled in one of the two parent studies, had documented breast or gynecologic cancer, were receiving matched or nonmatched therapy, and had completed TRSC and HRQOL-LASA instruments at least four weeks after initiation of the matched or nonmatched therapy but no longer than 12 weeks after therapy began. Power analysis (a priori) assuming a medium effect size and desired power of 0.8 for 13 independent variables identified that a minimum of 129 participants were needed for study analyses. Study procedures were reviewed and approved by the Avera Cancer Institute Institutional Review Board (IRB). The University of Kansas Medical Center’s IRB reviewed the study and relied on Avera Cancer Institute IRB approval.
Variables
Study variables were derived from concepts within the symptom management theory. Person-related variables included demographic (i.e., age and race/ethnicity) and socioeconomic (i.e., health insurance type and drug coverage) data. Health-/illness-related variables included therapy type (matched versus nonmatched), cancer type and stage, concurrent therapy type, length of current therapy, prior treatment modalities, timing of prior line of therapy, and comorbidities. Outcome variables were symptom occurrence and severity and HRQOL.
Symptom occurrence and severity were measured with the TRSC. The TRSC is a self-report instrument to assess the presence of 25 physical and psychological symptoms commonly experienced during cancer therapy. The severity of each symptom is also reported using a five-point Likert-type scale ranging from 0 (not present) to 4 (severe). Scores are summed to reflect the total TRSC score; a higher score indicates higher symptom occurrence and severity. Space exists at the bottom of the measure so that symptoms can be added if necessary; however, added symptoms are not included in the total TRSC score. Previous studies have reported Cronbach alphas ranging from 0.7–0.83 (Gonzalez, Williams, Tirado, & Williams, 2011; Heinze, 2012; Piamjariyakul et al., 2010; Williams et al., 2001). Strong inverse correlations (r = –0.32 to –0.45) with the Karnofsky Performance Status scale have demonstrated construct validity (Piamjariyakul et al., 2010; Williams, Balabagno, et al., 2010; Williams et al., 2001; Williams, Lopez, et al., 2010), and discriminant validity (80% correctly classified) has been shown in adult patients receiving chemotherapy versus radiation therapy (Williams et al., 2001; Williams, Lopez, et al., 2010).
The HRQOL-LASA measured HRQOL in this study. The HRQOL-LASA is a six-item questionnaire representing overall HRQOL and physical, emotional, mental, social, and spiritual well-being. Each item is self-rated on a 10-point Likert-type scale from 0 (as bad as it can be) to 10 (as good as it can be). Item scores are summed to reflect the total score; a high score indicates a high quality of life. Cronbach alpha has ranged from 0.83–0.93 in previous studies of patients with cancer (Heinze, 2012; Locke et al., 2007). Strong inverse correlations (r = –0.29 to –0.47) between total HRQOL-LASA and TRSC scores have also been reported, showing construct and discriminant validity (Heinze, 2012; Williams et al., 2013).
Data for this study were extracted from the electronic health record, with the exception of the TRSC and HRQOL-LASA data, which were obtained from the parent study files. Intra-rater reliability was established by re-extracting data from a random 10% of the sample. Data on therapy type were randomly reassessed on 20% of the sample. The audit revealed 100% agreement.
Data Analysis
Descriptive statistics were used to summarize sample characteristics and to report TRSC and HRQOL-LASA individual item scores and total scores. Independent-samples t tests were used to compare the mean individual item and total TRSC and HRQOL-LASA scores. Multiple linear regression analysis was performed to examine the association between therapy type and total TRSC score after controlling for person- and health-/illness-related variables, and to examine the association between therapy type and total HRQOL-LASA score after controlling for those variables. Dummy variables were created for cancer stage and the timing of prior line of therapy. Evaluation of model assumptions, including normality testing, evaluation of multicollinearity, and data independence, found no violation in these assumptions.
Linear regression modeling of the association between study variables and the total TRSC score was performed in two steps. Therapy type was added in the first step. Remaining study variables were added to the model in the second step. Modeling of the association between study variables and HRQOL was performed in three steps. Therapy type was added in the first step, person- and health-/illness-related variables were added in step two, and the total TRSC score was added in the final step. Two-tailed significance tests (F tests) for each step in the model were performed. In addition, t-test values and corresponding probability (p value), unstandardized B, and standard error of the estimate for each variable were determined. Level of significance for all analyses was set at alpha of 0.05 or less. Data analyses were performed using IBM SPSS Statistics, version 22.0.
Results
Sample Characteristics
Among the sample, 67 (52%) received matched therapy, and 62 (48%) received nonmatched therapy. The demographic and clinical profiles of the sample by therapy type are shown in Table 1. Patients receiving matched therapy were aged a mean of 56.6 years (SD = 12.1), and patients receiving nonmatched therapy were aged a mean of 55.4 years (SD = 13.4). The length of concurrent therapy was 6.8 weeks (SD = 2.3) for matched therapy and 7.6 weeks (SD = 2.3) for nonmatched therapy. Number of comorbidities was 2.2 (SD = 1.5) for patients receiving matched therapy and 2 (SD = 1.6) for patients receiving nonmatched therapy. Individuals receiving matched therapy had more prior lines of therapy (mean = 4.3, SD = 3.2) than those receiving nonmatched therapy (mean = 2.2, SD = 2.9). Drug coverage assistance outside of health insurance was necessary for a higher proportion of individuals receiving matched therapy (n = 25) compared to individuals receiving nonmatched therapy (n = 2). Most individuals receiving matched therapy were receiving targeted therapy plus chemotherapy (n = 37). Their combination varied across the sample by type of targeted therapy and type of chemotherapy. In addition, some individuals received more than one targeted therapy concomitantly. Table 2 shows the list of targeted therapy drugs used to match the genomic alterations found. The majority of individuals receiving nonmatched therapy received chemotherapy only (n = 39), most commonly taxane, anthracycline, and platinum-based drugs. More individuals receiving matched therapy had stage IV cancer (n = 30) than individuals receiving nonmatched therapy (n = 12). 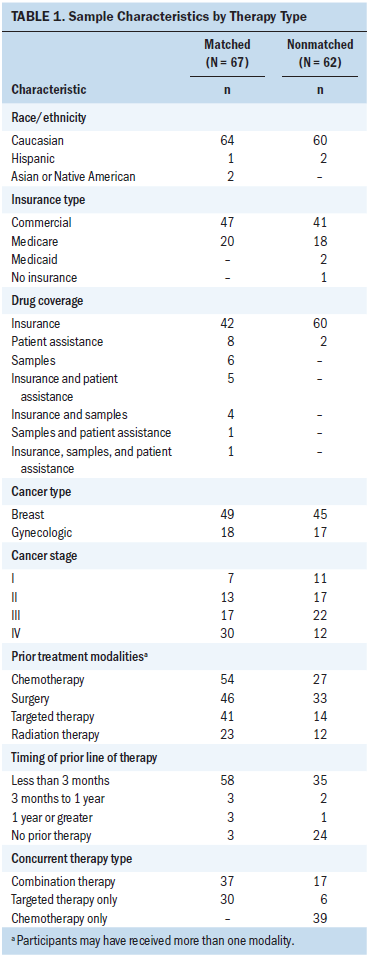
Therapy-Related Symptom Checklist Scores
The mean number of symptoms reported by individuals receiving matched therapy was 8 (SD = 4.9) as compared to a mean of 8.4 (SD = 5.2) reported by individuals receiving nonmatched therapy. Feeling sluggish was the highest occurring symptom in both groups. Numbness in fingers and/or toes was reported at a higher occurrence by individuals receiving matched therapy, but hair loss and difficulty concentrating were reported at higher occurrences by individuals receiving nonmatched therapy. The remaining symptoms on the TRSC were reported at similar rates of occurrence between groups. 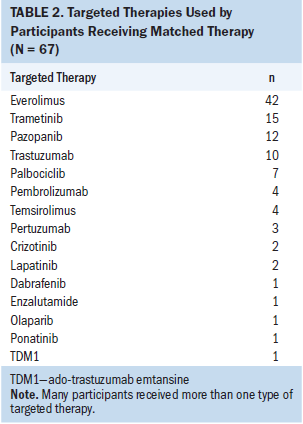
Regarding overall symptom occurrence and severity, the mean total TRSC score for individuals receiving matched therapy was 14.7 (SD = 10.1), which was lower than the mean total TRSC score for individuals receiving nonmatched therapy (mean = 16.1, SD = 11.6). However, the difference was not statistically significant (t[127] = 0.75, p = 0.45). Hair loss was the only symptom that was significantly different in terms of occurrence and severity score between the two groups (t[127] = 4, p ≤ 0.001). Table 3 shows the rank of occurrence for each of the 25 symptoms, the frequency of occurrence, and the mean rating of severity for each symptom by therapy type on the TRSC. The overall Cronbach alpha value for the TRSC was 0.83. 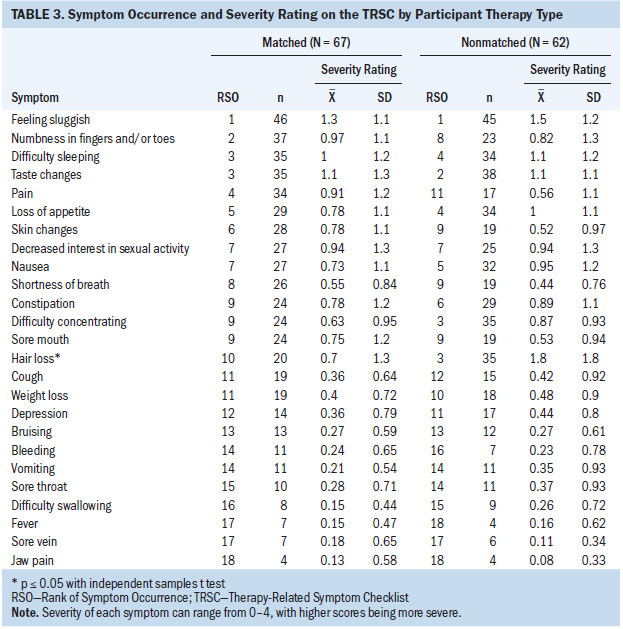
Fourteen individuals receiving matched therapy added symptoms to the TRSC as compared to 23 individuals receiving nonmatched therapy, which is much higher relative to past studies in which less than 2% of the sample added symptoms to the TRSC (Williams et al., 2013). Content analysis revealed that diarrhea was the most common symptom added in both groups, followed by vision changes and dry eyes.
Health-Related Quality of Life–Linear Analogue Self-Assessment Scores
The mean total HRQOL-LASA score for individuals receiving matched therapy was higher (mean = 48.1, SD = 7.5) than the mean score for individuals receiving nonmatched therapy (mean = 45.4, SD = 9.1); however, this was not statistically significant (t[127] = –1.89, p = 0.06). The level of social activity item response was significantly higher for individuals receiving matched therapy (t[127] = –2.91, p = 0.004). Table 4 shows the mean HRQOL-LASA total score and item responses. The Cronbach alpha for the HRQOL-LASA scores was 0.89. 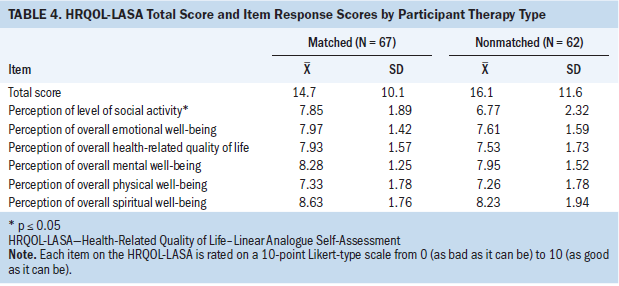
Multiple Linear Regression Modeling
Multiple linear regression modeling was used to determine the relationship between study variables and total TRSC scores (see Table 5) and revealed that less than 1% of the variance in symptom occurrence and severity was explained by therapy type alone (∆ R2 = 0.004, ∆ F = 0.57, p = 0.45), which was not statistically significant. The linear combination of all the variables in the model explained 10.3% of the variance in symptom occurrence and severity (∆ R2 = 0.1, ∆ F = 1.2, p = 0.35), which was not statistically significant. In the final model, individuals who had prior therapy less than three months before the onset of the therapy type had a significantly higher TRSC total score relative to individuals with no prior therapy (B = 6.2, p = 0.05). 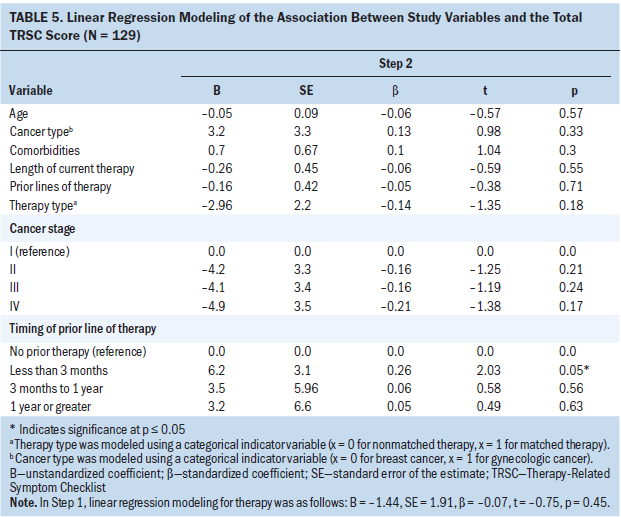
Multiple linear regression modeling to determine the relationship between study variables and total HRQOL-LASA scores (see Table 6) revealed that 3% of the variance in HRQOL was explained by therapy type (∆ R2 = 0.03, ∆ F = 3.6, p = 0.06), which was not statistically significant. The linear combination of all the variables in the model explained 33% of the variance in HRQOL, 20% of which was significantly explained by the TRSC score alone (∆ R2 = 0.2, ∆ F = 33.6, p ≤ 0.001). Individuals who had more prior lines of therapy had significantly higher HRQOL-LASA scores (B = 0.56, p = 0.05), and individuals who had higher TRSC scores had significantly lower HRQOL-LASA scores (B = –0.36, p ≤ 0.001) after controlling for all other variables in the model. 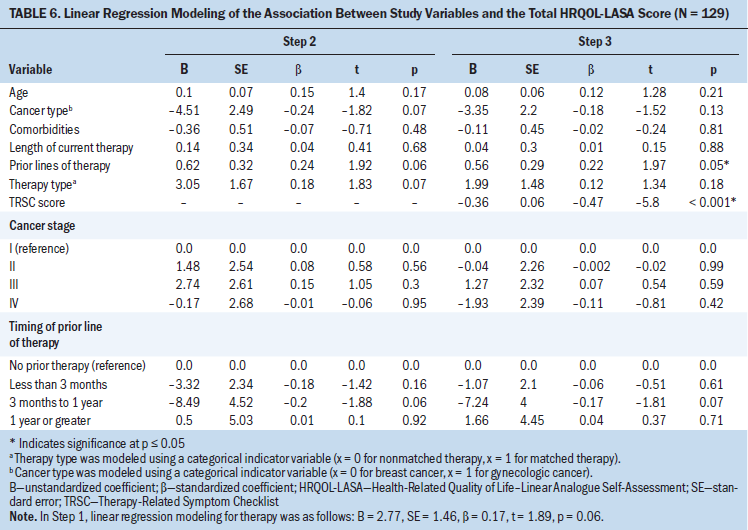
Discussion
Individuals receiving matched therapy had, on average, more prior lines of therapy and more advanced cancer, which is consistent with sample characteristics from other studies investigating the efficacy of matched therapy (André et al., 2014; Tsimeridou et al., 2012, 2014). It may be that these individuals failed traditional cancer therapies and were willing to try novel therapies (Rubin, 2015).
A large proportion of individuals receiving matched therapy required assistance outside of insurance to obtain drugs. This finding was understandable given the potential for off-label use of many of the targeted therapies. Although targeted therapies are developed to target a specific alteration that can be seen across a variety of cancer types, a drug’s indication is for a specific type of cancer. The U.S. Food and Drug Administration does not control provider decisions about which drugs can be prescribed; however, insurance companies frequently deny coverage when a drug is prescribed for an off-label use. This has contributed to larger, societal-wide discussions of the current feasibility of prescribing off-label use of drugs in the context of matched therapy (DeVita, Eggermont, Hellman, & Kerr, 2014; Gladwell, 2015; Mukherjee, 2016).
Symptoms
The average number of symptoms reported by individuals receiving matched and nonmatched therapy was similar. Results are comparable to the average number of symptoms reported during cancer treatment in other studies (Chen & Tseng, 2006; Janz et al., 2007); however, some studies have shown higher numbers of reported symptoms (Kenne-Sarenmalm, Ohlén, Jonsson, & Gaston-Johansson, 2007; Spichiger et al., 2011). Of note, different symptom scales were used in these studies.
The highest occurring symptom reported by both groups was feeling sluggish. Results parallel prior studies using the TRSC (Williams, Balabagno, et al., 2010; Williams, Mowlazadeh, Sisler, & Williams, 2015) and support the knowledge that fatigue is a common symptom experienced during cancer therapy (Abbott & Hooke, 2017). Numbness in fingers and/or toes was reported more often by individuals receiving matched therapy who, as a group, also had more prior lines of therapy. This is consistent with findings of significantly higher levels of neuropathy among individuals who previously received chemotherapy (Lewis et al., 2015). Individuals receiving nonmatched therapy more frequently reported difficulty concentrating even though they received fewer lines of therapy than individuals on matched therapy. Cognitive impairments, such as difficulty concentrating, are commonly experienced during cancer treatment (Von Ah et al., 2016) and have been linked to multiple factors, including chemotherapy and anxiety (Janelsins et al., 2017). Because individuals receiving nonmatched therapy had less experience with cancer treatment, they may have felt increased anxiety about their treatment and, therefore, increased difficulty concentrating.
Average total TRSC scores were lower for individuals receiving matched therapy compared to individuals receiving nonmatched therapy; however, this difference did not achieve statistical significance. Lower scores may have been related to prior experience with therapy-related symptoms and subsequent increased proficiency at managing symptoms, a concept that is supported by other studies (Duijts, Faber, Oldenburg, van Beurden, & Aaronson, 2011; Given et al., 2002; Williams et al., 2013). Total TRSC scores for individuals receiving nonmatched therapy were similar to TRSC scores in other studies (Piamjariyakul et al., 2010; Williams, Lopez, et al., 2010; Williams, Williams, LaFaver-Roling, Johnson, & Williams, 2011). Significantly higher TRSC scores for hair loss were reported by individuals receiving nonmatched therapy, which was not surprising because hair loss is a known side effect of chemotherapies commonly used to treat breast and gynecologic cancers.
A substantial number of individuals added symptoms to the TRSC compared to prior studies, suggesting the TRSC may not fully capture the symptoms related to current therapies. More individuals receiving nonmatched therapy added symptoms, which was unexpected because individuals receiving matched therapy were often receiving novel drug combinations. Results may suggest that symptoms are not markedly different between matched or nonmatched therapy or that symptoms are not fully captured on the TRSC. Future studies should determine the adequacy of symptom assessment tools in the context of matched therapy in a broader population.
Health-Related Quality of Life
Average HRQOL-LASA scores were higher for individuals receiving matched therapy compared to individuals receiving nonmatched therapy; however, the difference in scores was not statistically significant. Individuals receiving matched therapy had lower average TRSC scores, which is consistent with other studies showing an inverse relationship between TRSC and HRQOL-LASA scores (Gonzalez et al., 2011; Heinze, 2012; Williams et al., 2013). Hope gained from a novel treatment may have influenced HRQOL for individuals receiving matched therapy. Prior studies have found that continuing cancer treatment allowed individuals to feel hopeful about their HRQOL and longer survival and that their biggest fear was being told there were no other treatment options (Luoma & Hakamies-Blomqvist, 2004; Sarenmalm, Thorén-Jönsson, Gaston-Johansson, & Ohlén. 2009).
Individuals receiving matched therapy reported significantly higher scores on the social domain item, even though they were more likely to have advanced cancer. Other studies have found patients with cancer are more intentional with their social activities and relationships and that social support was an important influence on HRQOL (Leung, Pachana, & McLaughin, 2014; Park, Bae, Jung, & Kim, 2012).
Associations Among Therapy Type, Symptoms, and Health-Related Quality of Life
Therapy type was not significantly associated with symptom occurrence and severity and only explained 1% of the variance in symptom occurrence and severity. This finding provides initial evidence that, in this sample, matched therapy elicited little change to the symptom experience despite the frequent use of novel drug combinations. Individuals who had received therapy less than three months before the onset of their current therapy had significantly higher TRSC scores compared to those who had no prior therapy. This finding was not unexpected, but a review of the literature failed to describe this relationship. Results suggest it is a variable warranting inclusion in future studies.
The overall model explained 10% of the variance in symptom occurrence and severity, suggesting the symptom experience is a complex process. Other influencing variables were not accounted for in this study. The side effect profile for each therapy/combination of therapy may have influenced TRSC scores. However, the study was insufficiently powered to account for every therapy combination in the regression analysis.
Therapy type was not significantly associated with HRQOL and explained 3% of the variance in HRQOL-LASA scores alone. Findings provide initial data documenting the effect of matched therapy on HRQOL. Understanding the efficacy of new cancer treatments and patient-reported outcomes, such as HRQOL, is crucial to have meaningful discussions about specific therapy-related risks and benefits (Osaba, 2011). Person- and health-/illness-related variables explained 11% of the variance in HRQOL modeling, and the addition of the TRSC scores explained 20% of the total variance in HRQOL. Results are similar to a study by Janz et al. (2007) that found symptom burden to be the most influential variable on HRQOL after controlling for person- and health-/illness-related variables among individuals with breast cancer. Other studies have confirmed significant associations between a higher symptom burden and poorer HRQOL (Huang et al., 2013; Miaskowski et al., 2006; Smith et al., 2013); however, different symptom and HRQOL scales were used in these studies. A higher number of prior lines of therapy was associated with a higher HRQOL, but this finding should be interpreted with caution because the p value was 0.05. This was an unexpected finding and may reflect proficiencies gained with managing symptoms, which may influence HRQOL.
Symptom Management Theory Framework
Results from this study provided support for the relationship between certain health-/illness-related factors and the symptom experience as identified in the symptom management theory and can serve as a hypothesis-generating study for future research. Specifically, a significant relationship between the timing of the prior line of therapy and symptom occurrence and severity was found. Also consistent with the symptom management theory, a significant relationship between the symptom experience and HRQOL was confirmed in this study. The health-/illness-related variable of number of prior lines of therapy was significantly associated with HRQOL, which may suggest that the symptom management strategies concept of the symptom management theory can influence HRQOL. The symptom management strategies concept relates to the interventional approaches taken to alleviate symptoms experienced by the individual to achieve the desired outcome (Dodd et al., 2001). Findings may indicate that individuals receiving more prior lines of therapy had more experience with effective symptom management strategies; this should be examined in future studies. The symptom experience and HRQOL are complex concepts with many influencing factors; therefore, future research should reexamine the links among the symptom management theory concepts and examine potentially important mediator and moderator variables.
Limitations
The retrospective, correlational design and the cross-sectional nature of the data limits the study to assessment of association rather than causation. Longitudinal assessments are recommended for future studies to better characterize influences of therapy type on symptoms and HRQOL. Symptoms and HRQOL were unknown prior to starting therapy; therefore, potentially significant differences at baseline may have existed. The homogenous ethnic sample limits the generalizability of the study, and future studies should consider a more diverse population. The type of concurrent therapy and/or the type of prior lines of therapy may have influenced TRSC and HRQOL-LASA scores, which were not included in the regression analyses.
Implications for Nursing
Nursing science is concerned with the human response to illness, making symptoms and HRQOL important areas to study. Survival benefits of matched therapy are being investigated; therefore, the effect of this therapy on the individual is a timely research endeavor. Results from this study provide foundational evidence of the symptom experience and HRQOL in individuals receiving matched therapy. Future efforts to build upon these results will provide a better understanding of the symptoms and potential effects on HRQOL for individuals receiving matched therapy and for the nurses caring for them. This information is essential to provide anticipatory guidance on therapy-related symptoms and education about symptom management. Nursing science must continue to generate new knowledge related to symptoms and HRQOL in the context of state-of-the-art cancer care to improve the well-being of individuals with cancer. [[{"fid":"47396","view_mode":"default","fields":{"format":"default","alignment":"","field_file_image_alt_text[und][0][value]":false,"field_file_image_title_text[und][0][value]":false},"link_text":null,"type":"media","field_deltas":{"1":{"format":"default","alignment":"","field_file_image_alt_text[und][0][value]":false,"field_file_image_title_text[und][0][value]":false}},"attributes":{"class":"media-element file-default","data-delta":"1"}}]]
Conclusion
This study was conducted to develop an understanding of the symptom experience and HRQOL for individuals receiving matched therapy. Additional research focused on the symptom experience and effects on HRQOL in the context of matched therapy is needed. This includes investigating important links between symptoms and HRQOL, identifying mediating and moderating factors, and ensuring that symptoms are being adequately captured with existing tools. Future research would benefit from a mixed-methods approach to explore perceptions about matched therapy, symptoms, effects on HRQOL, and symptom management strategies. If precision medicine intends to tailor treatment to the individual, then future research should consider ways to tailor care as well.
The authors gratefully acknowledge Phoebe D. Williams, PhD, RN, FAAN, for her initial guidance on the study concept. They also thank the patients, their families, and the research staff at the Avera Cancer Institute.
About the Author(s)
Kirstin Williams, PhD, CNP, is a clinician scientist and nurse practitioner at the Avera Cancer Institute in Sioux Falls, SD, and a postdoctoral fellow in the School of Nursing at the University of Kansas in Kansas City; and Sandra Bergquist-Beringer, PhD, RN, CWCN, is a professor in the School of Nursing at the University of Kansas Medical Center in Kansas City. The authors take full responsibility for this content. This research was funded, in part, by the Crighton Scholar Award and the Sousa Scholar Award. Williams contributed to the conceptualization and design, completed the data collection, and provided statistical support. Both authors provided the analysis and contributed to the manuscript preparation. Williams can be reached at kirstin.williams@avera.org, with copy to ONFEditor@ons.org. (Submitted October 2017. Accepted May 3, 2018.)
References
Abbott, L., & Hooke, M.C. (2017). Energy Through Motion: An activity intervention for cancer-related fatigue in an ambulatory infusion center. Clinical Journal of Oncology Nursing, 21, 618–626. https://doi.org/10.1188/17.CJON.618-626
American Cancer Society. (2018). Cancer facts and figures, 2018. Retrieved from https://bit.ly/2B7HxgY
André, F., Bachelot, T., Commo, F., Campone, M., Arnedos, M., Dieras, V., . . . Bonnefoi, H. (2014). Comparative genomic hybridization array and DNA sequencing to direct treatment of metastatic breast cancer: A multicenter, prospective trial (SAFIR01/UNICANCER). Lancet Oncology, 15, 267–274. https://doi.org/10.1016/S1470-2045(13)70611-9
Chen, M.L., & Tseng, H.C. (2006). Symptom clusters in cancer patients. Supportive Care in Cancer, 14, 825–830. https://doi.org/10.1007/s00520-006-0019-8
Cleeland, C.S. (2000). Cancer-related symptoms. Seminars in Radiation Oncology, 10, 175–190.
DeVita, V.T., Jr., Eggermont, A.M., Hellman, S., & Kerr, D.J. (2014). Clinical cancer research: The past, present and the future. Nature Reviews Clinical Oncology, 11, 663–669. https://doi.org/10.1038/nrclinonc.2014.153
Dodd, M., Janson, S., Facione, N., Faucett, J., Froelicher, E.S., Humphreys, J., . . . Taylor, D. (2001). Advancing the science of symptom management. Journal of Advanced Nursing, 33, 668–676. https://doi.org/10.1046/j.1365-2648.2001.01697.x
Duijts, S.F., Faber, M.M., Oldenburg, H.S., van Beurden, M., & Aaronson, N.K. (2011). Effectiveness of behavioral techniques and physical exercise on psychosocial functioning and health-related quality of life in breast cancer patients and survivors—A meta-analysis. Psycho-Oncology, 20, 115–126. https://doi.org/10.1002/pon.1728
Dy, G.K., & Adjei, A.A. (2013). Understanding, recognizing, and managing toxicities of targeted anticancer therapies. CA: A Cancer Journal for Clinicians, 63, 249–279. https://doi.org/10.3322/caac.21184
Given, B., Given, C.W., McCorkle, R., Kozachik, S., Cimprich, B., Rahbar, M.H., . . . Wojcik, C. (2002). Pain and fatigue management: Results of a nursing randomized clinical trial. Oncology Nursing Forum, 29, 949–956. https://doi.org/10.1188/02.ONF.949-956
Gladwell, M. (2015, December 14). Tough medicine: A disturbing report from the front lines of the war on cancer. The New Yorker. Retrieved from http://www.newyorker.com/magazine/2015/12/14/tough-medicine
Gonzalez, V., Williams, P.D., Tirado, M., & Williams, D.D. (2011, March). Patient-reported symptoms, alleviation and self-care methods, daily activities, and health-related quality of life during outpatient cancer treatments in Puerto Rico. Poster presented at the Midwest Nursing Research Society Conference, Columbus, OH.
Heinze, S.B. (2012). Relationships among symptoms, brain-derived neurotrophic factor (BDNF), daily activities, self-care, and quality of life in breast cancer survivors. (Doctoral dissertation). Retrieved from https://kuscholarworks.ku.edu/handle/1808/11445?show=full
Huang, H.Y., Tsai, W.C., Chou, W.Y., Hung, Y.C., Liu, L.C., Huang, K.F., . . . Kung, P.T. (2017). Quality of life of breast and cervical cancer survivors. BMC Women’s Health, 17, 30. https://doi.org/10.1186/s12905-017-0387-x
Huang, S.M., Tai, C.J., Lin, K.C., Tai, C.J., Tseng, L.M., & Chien, L.Y. (2013). A comparative study of symptoms and quality of life among patients with breast cancer receiving target, chemotherapy, or combined therapy. Cancer Nursing, 36, 317–325. https://doi.org/10.1097/NCC.0b013e318268f86d
Janelsins, M.C., Heckler, C.E., Peppone, L.J., Kamen, C., Mustian, K.M., Mohile, S.G., . . . Morrow, G.R. (2017). Cognitive complaints in survivors of breast cancer after chemotherapy compared with age-matched controls: An analysis from a nationwide, multicenter, prospective longitudinal study. Journal of Clinical Oncology, 35, 506–514. https://doi.org/10.1200/JCO.2016.68.5826
Janz, N.K., Mujahid, M., Chung, L.K., Lantz, P.M., Hawley, S.T., Morrow, M., . . . Katz, S.J. (2007). Symptom experience and quality of life of women following breast cancer treatment. Journal of Women’s Health, 16, 1348–1361. https://doi.org/10.1089/jwh.2006.0255
Kenne-Sarenmalm, E., Ohlén, J., Jonsson, T., & Gaston-Johansson, F. (2007). Coping with recurrent breast cancer: Predictors of distressing symptoms and health-related quality of life. Journal of Pain and Symptom Management, 34, 24–39. https://doi.org/10.1016/j.jpainsymman.2006.10.017
Kirkova, J., Aktas, A., Walsh, D., & Davis, M.P. (2011). Cancer symptom clusters: Clinical and research methodology. Journal of Palliative Medicine, 14, 1149–1166. https://doi.org/10.1089/jpm.2010.0507
Kirkova, J., Walsh, D., Rybicki, L., Davis, M.P., Aktas, A., Tao, J., & Homsi, J. (2010). Symptom severity and distress in advanced cancer. Palliative Medicine, 24, 330–339. https://doi.org/10.1177/0269216309356380
Kluetz, P.G., Chingos, D.T., Basch, E.M., & Mitchell, S.A. (2016). Patient-reported outcomes in cancer clinical trials: Measuring symptomatic adverse events with the National Cancer Institute’s patient-reported outcomes version of the common terminology criteria for adverse events (PRO-CTCAE). American Society of Clinical Oncology Educational Book, 35, 67–73. https://doi.org/10.14694/EDBK_159514
Leung, J., Pachana, N.A., & McLaughin, D. (2014). Social support and health-related quality of life in women with breast cancer: A longitudinal study. Psycho-Oncology, 23, 1014–1020. https://doi.org/10.1002/pon.3523
Lewis, M.A., Zhao, F., Jones, D., Loprinzi, C.L., Brell, J., Weiss, M., & Fisch, M.J. (2015). Neuropathic symptoms and their risk factors in medical oncology outpatients with colorectal vs. breast, lung, or prostate cancer: Results from a prospective multicenter study. Journal of Pain and Symptom Management, 49, 1016–1024. https://doi.org/10.1016/j.jpainsymman.2014.11.300
Locke, D.E., Decker, P.A., Sloan, J.A., Brown, P.D., Malec, J.F., Clark, M.M., . . . Buckner, J.C. (2007). Validation of single-item linear analog scale assessment of quality of life in neuro-oncology patients. Journal of Pain and Symptom Management, 34, 628–638. https://doi.org/10.1016/j.jpainsymman.2007.01.016
Luoma, M.L., & Hakamies-Blomqvist, L. (2004). The meaning of quality of life in patients being treated for advanced breast cancer: A qualitative study. Psycho-Oncology, 13, 729–739. https://doi.org/10.1002/pon.788
Miaskowski, C., Barsevick, A., Berger, A., Casagrande, R., Grady, P.A., Jacobsen, P., . . . Marden, S. (2017). Advancing symptom science through symptom cluster research: Expert panel proceedings and recommendations. Journal of the National Cancer Institute, 109(4). https://doi.org/10.1093/jnci/djw253
Miaskowski, C., Cooper, B.A., Paul, S.M., Dodd, M., Lee, K., Aouizerat, B.E., . . . Bank, A. (2006). Subgroups of patients with cancer with different symptom experiences and quality-of-life outcomes: A cluster analysis [Online exclusive]. Oncology Nursing Forum, 33, E79–E89. https://doi.org/10.1188/06.ONF.E79-E89
Mukherjee, S. (2016, May 12). The improvisational oncologist. New York Times. Retrieved from https://www.nytimes.com/2016/05/15/magazine/oncologist-improvisation.ht…
National Cancer Institute. (2018). Targeted cancer therapies. Retrieved from https://www.cancer.gov/about-cancer/treatment/types/targeted-therapies/…
Nikanjam, M., Liu, S., & Kurzrock, R. (2016). Dosing targeted and cytotoxic two-drug combinations: Lessons learned from analysis of 24,326 patients reported 2010 through 2013. International Journal of Cancer, 139, 2135–2141. https://doi.org/10.1002/ijc.30262
Osaba, D. (2011). Health-related quality of life and cancer clinical trials. Therapeutic Advances in Medical Oncology, 3(2), 57–71. https://doi.org/10.1177/1758834010395342
Park, J.H., Bae, S.H., Jung, Y.S., & Kim, K.S. (2012). Quality of life and symptom experience in breast cancer survivors after participating in a psychoeducational support program: A pilot study. Cancer Nursing, 35(1), E34–E41. https://doi.org/10.1097/NCC.0b013e318218266a
Piamjariyakul, U., Williams, P.D., Prapakorn, S., Kim, M., Park, L., Rojjanansrirat, W., & Williams, A.R. (2010). Cancer therapy-related symptoms and self-care in Thailand. European Journal of Oncology Nursing, 14, 387–394. https://doi.org/10.1016/j.ejon.2010.01.018
Reeve, B.B., Mitchell, S.A., Dueck, A.C., Basch, E., Cella, D., Reilly, C.M., . . . Bruner, D.W. (2014). Recommended patient-reported core set of symptoms to measure in adult cancer treatment trials. Journal of the National Cancer Institute, 106(7), pii: dju129. https://doi.org/10.1093/jnci/dju129
Rubin, R. (2015). Experts critical of America’s right-to-try drug laws. Lancet, 386, 1325–1326. https://doi.org/10.1016/S0140-6736(15)00393-1
Sarenmalm, E.K., Thorén-Jönsson, A.L., Gaston-Johansson, F., & Ohlén, J. (2009). Making sense of living under the shadow of death: Adjusting to a recurrent breast cancer illness. Qualitative Health Research, 19, 1116–1130. https://doi.org/10.1177/1049732309341728
Schwaederle, M., Daniels, G.A., Piccioni, D.E., Kesari, S., Fanta, P.T., Schwab, R.B., . . . Kurzrock, R. (2015). Next generation sequencing demonstrates association between tumor suppressor gene aberrations and poor outcome in patients with cancer. Cell Cycle, 14, 1730–1737. Retrieved from https://doi.org/10.1080/15384101.2015.1033596
Schwaederle, M., Parker, B.A., Schwab, R.B., Daniels, G.A., Piccioni, D.E., Kesari, S., . . . Kurzrock, R. (2016). Precision oncology: The UC San Diego Moores Cancer Center PREDICT experience. Molecular Cancer Therapeutics, 15, 743–752. https://doi.org/10.1158/1535-7163.MCT-15-0795
Smith, A.W., Bellizzi, K.M., Keegan, T.H., Zebrack, B., Chen, V.W., Neale, A.V., . . . Lynch, C.F. (2013). Health-related quality of life of adolescent and young adult patients with cancer in the United States: The adolescent and young adult health outcomes and patient experience study. Journal of Clinical Oncology, 31, 2136–2145. https://doi.org/10.1200/JCO.2012.47.3173
Smith, S.G., Sestak, I., Howell, A., Forbes, J., & Cuzick, J. (2017). Participant-reported symptoms and their effect on long-term adherence in the international breast cancer intervention study I (IBIS I). Journal of Clinical Oncology, 35, 2666–2673. https://doi.org/10.1200/JCO.2016.71.7439
Spichiger, E., Muller-Frohlich, C., Denhaerynch, K., Stoll, H., Hantikainen, V., & Dodd, M. (2011). Prevalence of symptoms, with a focus on fatigue, and changes of symptoms over three months in outpatients receiving chemotherapy. Swiss Medical Weekly, 141, w13303. https://doi.org/10.4414/smw.2011.13303
Tsimberidou, A.M., Iskander, N.G., Hong, D.S., Wheler, J.J., Falchook, G.S., Fu, S., . . . Kurzrock, R. (2012). Personalized medicine in a phase I clinical trials program: The MD Anderson Cancer Center initiative. Clinical Cancer Research, 18, 6373–6383. https://doi.org/10.1158/1078-0432.CCR-12-1627
Tsimberidou, A.M., Wen, S., Hong, D.S., Wheler, J.J., Falchook, G.S., Fu, S., . . . Berry, D. (2014). Personalized medicine for patients with advanced cancer in the phase I program at MD Anderson: Validation and landmark analyses. Clinical Cancer Research, 20, 4827–4836. https://doi.org/10.1158/1078-0432.CCR-14-0603
U.S. Food and Drug Administration. (2017). Precision medicine. Retrieved from https://www.fda.gov/medicaldevices/productsandmedicalprocedures/invitro…
Von Ah, D., Storey, S., Tallman, E., Nielsen, A., Johns, S.A., & Pressler, S.J. (2016). Cancer, cognitive impairment, and work-related outcomes: An integrative review. Oncology Nursing Forum, 43, 602–616. https://doi.org/10.1188/16.ONF.602-616
Williams, A.R., Mowlazadeh, B., Sisler, L., & Williams, P.D. (2015). Self-reported assessment of symptoms and self-care within a cohort of U.S. veterans during outpatient care for cancer. Clinical Journal of Oncology Nursing, 19, 595–602. https://doi.org/10.1188/15.CJON.595-602
Williams, P.D., Balabagno, A.O., Manahan, L., Piamjariyakul, U., Ranallo, L., Laurente, C.M., . . . Williams, A.R. (2010). Symptom monitoring and self-care practices among Filipino cancer patients. Cancer Nursing, 33, 37–46. https://doi.org/10.1097/NCC.0b013e3181b0f2b4
Williams, P.D., Ducey, K.A, Sears, A.M., Williams, A.R., Tobin-Rumelhart, S.E., & Bunde, P. (2001). Treatment type and symptom severity among oncology patients by self-report. International Journal of Nursing Studies, 38, 359–367.
Williams, P.D., Graham, K.M., Storlie, D.L., Pedace, T.M., Haeflinger, K.V., Williams, D.D., . . . Williams, A.R. (2013). Therapy-related symptom checklist use during treatments at a cancer center. Cancer Nursing, 36, 245–254. https://doi.org/10.1097/NCC.0b013e3182595406
Williams, P.D., Lopez, V., Ying, C.S., Piamjariyakul, U., Wenru, W., Hung, G.T., . . . Williams, A.R. (2010). Symptom monitoring and self-care practices among oncology adults in China. Cancer Nursing, 33, 185–193. https://doi.org/10.1097/NCC.0b013e3181c29598
Williams, P.D., Williams, K., LaFaver-Roling, S., Johnson, R., & Williams, A.R. (2011). An intervention to manage patient-reported symptoms during cancer treatment. Clinical Journal of Oncology Nursing, 15, 253–258. https://doi.org/10.1188/11.CJON.253-258


