A Distress Thermometer Intervention for Patients With Head and Neck Cancer
Objectives: To investigate the feasibility of an intervention using the National Comprehensive Cancer Network Distress Thermometer and Problem List with nurse-guided follow-up and the effect on depressive symptoms, health-related quality of life, and worry of cancer in patients with head and neck cancer.
Sample & Setting: 110 patients with head and neck cancer in a two-arm randomized, controlled trial in an outpatient clinic of a university hospital.
Methods & Variables: Patients were randomized to usual care (n = 57) or the intervention group (n = 53), which consisted of screening with the Distress Thermometer and Problem List plus nurse-guided follow-up lasting about 20 minutes three to four times during 12 months. Intention-to-treat analysis was performed using linear mixed models with outcomes at 6 and 12 months and baseline adjustment.
Results: The intervention showed moderate compliance and acceptable session duration. Intervention participants were satisfied with nurses’ care. Depressive symptoms, health-related quality of life, and worry of cancer were not significantly different in the two treatment groups. The intervention seemed feasible in clinical practice, but no effects on patient outcomes were seen.
Implications for Nursing: Patients with head and neck cancer appreciated the opportunity to discuss their problems and challenges with a nurse. Nurses supported patients with basic psychosocial care, minor interventions, and referral possibilities.
Jump to a section
Dependent on the location of the tumor and the type of treatment, patients with head and neck cancer (HNC) are prone to physical problems like dry mouth (Jiang, Zhao, Jansson, Chen, & Mårtensson, 2017), impaired speech (Heijnen et al., 2016; Rinkel et al., 2016), difficulty eating (Ottosson, Laurell, & Olsson, 2013), or altered shoulder function (Rogers et al., 2016). In many patients, the physical problems are visible and have a strong negative impact on diverse functions and psychosocial well-being (Semple, Dunwoody, Kernohan, McCaughan, & Sullivan, 2008). Although physical problems can improve in the period directly after end of treatment, many problems are irreversible and persist in the long-term. Partly because of the long-lasting physical problems, patients often suffer from distress.
Patients with HNC are at higher risk and suffer from greater distress than patients diagnosed with any other form of cancer because of the effect of impairments in functioning (Ahn et al., 2015; Singer et al., 2012). From 35%–41% of patients with HNC experience high levels of distress pre- and post-treatment up to one year after treatment (Buchmann, Conlee, Hunt, Agarwal, & White, 2013; Ninu et al., 2016). In Dutch patients, a prevalence rate of 29% was found during follow-up care (Krebber, Jansen, Cuijpers, Leemans, & Verdonck-de Leeuw, 2016). A variable related to distress is depressive symptoms (Dunne et al., 2017), which are present in 28%–39% of patients at diagnosis (de Leeuw, de Graeff, Ros, Hordijk, et al., 2000) and persists in 20% of patients after one year (de Leeuw, de Graeff, Ros, Blijham, et al., 2000). Depressive symptoms at diagnosis are known to be predictive of a poor health-related quality of life (HRQOL) one to three years later (Hammerlid, Silander, Hörnestam, & Sullivan, 2001; Ronis, Duffy, Fowler, Khan, & Terrell, 2008). In addition, poor HRQOL is associated with high levels of distress (Bornbaum et al., 2012; Dunne et al., 2017; Ninu et al., 2016; Pandey, Devi, Ramdas, Krishnan, & Kumar, 2009). Patients with HNC experience deterioration of HRQOL directly after the start of treatment (Rogers, Ahad, & Murphy, 2007), which can persist for as many as 10 years after completion of treatment (Mehanna & Morton, 2006; Oskam et al., 2013). High levels of distress are also related to fear of cancer recurrence (Dunne et al., 2017; Simonelli, Siegel, & Duffy, 2016; Van Liew, Christensen, Howren, Hynds Karnell, & Funk, 2014), which can persist as many as three years after treatment (Rogers et al., 2009). About 20% of patients with HNC experience a recurrence, of which 90% happen in the first two years after treatment (Kissun et al., 2006).
Therefore, additional care is needed to support patients in the period after completion of cancer treatment to decrease physical problems, to learn to cope with these problems, and to lower distress. Screening for distress has become a more standard practice besides the regular medical post-treatment care. A frequently used scale for distress screening is the National Comprehensive Cancer Network Distress Thermometer (DT), often combined with the Problem List (PL). The DT is first mentioned in literature by Roth et al. (1998). The DT is a visual analog scale that measures emotional distress, and the PL assesses practical, family, emotional, religious or spiritual, and physical problems. Although the PL is designed for patients with cancer in general, it also addresses specific problems experienced by patients with HNC, such as dry mouth.
The DT&PL has been referred to in more than 200 publications in diverse cancer populations, including patients with HNC (Buchmann et al., 2013; Ghazali et al., 2017; Ninu et al., 2016). Many studies have focused on the validity of the DT&PL (Snowden et al., 2011), prevalence of distress (Lester et al., 2015; Petty & Lester, 2014), detection of reliable cutoff points (Ma et al., 2014), appropriate time points for screening (Ploos van Amstel et al., 2013), improvement of communication (Braeken et al., 2013; Mitchell, 2013), or translation into diverse languages (Donovan, Grassi, McGinty, & Jacobsen, 2014). However, studies focusing on the effect of screening with the DT&PL, including referral on distress or related patient outcomes, are scant. A study protocol in patients with breast cancer (Ploos van Amstel, Prins, van der Graaf, Peters, & Ottevanger, 2016) and a randomized, controlled trial in patients with cancer starting radiation therapy or chemotherapy (Hollingworth et al., 2013) have been published. In Hollingworth et al.’s (2013) study, the intervention group completed the DT&PL and discussed sources of distress with a trained radiographer/nurse, and outcomes were compared to standard care. No beneficial effects were found on distress, HRQOL, or healthcare costs. Of note, 33% of the patients experienced high levels of distress, but less than 3% were referred to a clinical psychologist (Hollingworth et al., 2013). Another randomized, controlled trial of 3,133 newly diagnosed outpatients with cancer evaluated computerized versus personal triage with several screening questionnaires, including the DT&PL. Results showed a decrease in distress in the intervention and control groups as many as 12 months postdiagnosis. The authors stated that this main effect was related to participants who accepted referral regardless of group, and more research is needed to explore ways to improve uptake of resources (Carlson, Waller, Groff, Zhong, & Bultz, 2012).
A lack of evidence exists for a relationship between screening for distress (including referral possibilities) and a decrease in distress (Carlson, Waller, & Mitchell, 2012; Hollingworth et al., 2013; Meijer et al., 2013). Therefore, more research is needed to improve the effectiveness of the DT&PL. Because referral rates are low even in patients experiencing distress (Bauwens, Baillon, Distelmans, & Theuns, 2014; Hollingworth et al., 2013; Verdonck-de Leeuw et al., 2009), the authors of the current study added a short nurse-guided follow-up session to screening with the DT&PL to create the DT&PL+ intervention.
The aim of this study was to investigate the feasibility of the DT&PL+ intervention and its effectiveness on depressive symptoms (primary outcome), HRQOL, and fear of cancer recurrence in patients with HNC. The authors hypothesized that, one year after inclusion, patients with HNC in the intervention group would report fewer depressive symptoms, better HRQOL, fewer physical symptoms, and less fear of cancer recurrence than patients with HNC in the control group.
Methods
Design and Sample
To evaluate the feasibility and the effectiveness of the DT&PL+ intervention, a two-arm randomized, controlled trial was conducted. The sample consisted of patients who visited the outpatient clinic of oral maxillofacial and otorhinolaryngology of the University Medical Center Utrecht in the Netherlands before and as long as six months after cancer treatment. Inclusion criteria were diagnosis of squamous cell carcinoma of the oral cavity, oropharynx, hypopharynx, or larynx; ability to complete questionnaires in Dutch; and ability to participate in the intervention. Because the DT&PL is meant for the total cancer population, a history of depression was not an exclusion criterion.
Procedures
Participants were enrolled by the physician from April to September 2012. The study was performed preceding the implementation of the DT&PL+ intervention as standard care at the outpatient clinic.
Each patient received verbal and written information about the study. After giving their informed consent, participants were randomized to the DT&PL+ intervention or usual care using a block procedure, stratified by gender, cancer site (oral/oropharyngeal cancer versus hypopharyngeal/laryngeal cancer), and treatment status (new patients, 0–3 months after cancer treatment, and 0–6 months after cancer treatment).
All participants were asked to complete questionnaires at baseline (i.e., 0–6 months after cancer treatment) (M1) and at 6 months (M2) and 12 months (M3) after baseline. Participants received the questionnaires at home and returned them using a prepaid return envelope. The study was reviewed and registered by the medical ethics committee of the University Medical Center Utrecht (No. 12-029/C). Participants could withdraw their consent at any time without giving a reason.
Usual Care
Patients received care provided by their HNC specialist or physician at two-month intervals in the first year after cancer treatment and at two-month intervals in the second year. The 10-minute appointments were primarily aimed at the treatment of complications and the detection of recurrences or secondary primary tumors. No formal time was reserved to discuss the patients’ psychosocial concerns. However, if the patient was considered to be in need of psychosocial support, the HNC specialist could refer the patient to psychosocial care.
Intervention
The DT&PL+ intervention consisted of screening for distress combined with a short nurse-guided follow-up to identify distress in patients with HNC, with a goal of providing immediate support, advice, information, or referral if necessary. The DT measures the severity of distress on a 0–10 visual analog scale shaped like a thermometer. The DT has been validated and is sensitive (0.85) and specific (0.67) in Dutch patients with cancer, including patients with HNC (Tuinman, Gazendam-Donofrio, & Hoekstra-Weebers, 2008). A score of 5 or greater was considered to be an elevated distress score for this study (Tuinman et al., 2008). The DT is used in conjunction with the PL, which assesses 47 items in categories of practical, family, emotional, religious or spiritual, and physical (http://bit.ly/1SMfIew). The patient can select whether or not he or she experiences each of the 47 items. The PL has been validated and shows a good internal consistency (Cronbach alpha = 0.9) (Tuinman et al., 2008). At the end of the PL, there is a question that asks whether the patient would like to talk to a professional about his or her problems, which can be answered with yes, maybe, or no.
The intervention consisted of three to four 20-minute sessions during one year. An intervention session contains three components. First, the patient completes the DT&PL at home and brings it to the outpatient clinic. Second, regardless of the DT&PL score, the patient has an appointment with a trained nurse directly after his or her medical appointment with the HNC specialist at the outpatient clinic. The general outcome of the DT&PL is discussed, and specific problems are identified in dialogue with the patient. Third, if indicated, basic psychosocial care, minor nursing interventions, or referral to other healthcare providers or patient programs was arranged.
Basic psychosocial care encompasses providing education about the disease and its treatment, providing emotional support, attempting to resolve symptoms and complaints, providing support in regard to making decisions about treatment possibilities, and arranging referral based on observed problems. Minor nursing interventions include prescribing mouth gel or giving advice about supplementary feeding. The outcome of the DT&PL, important details, and the care provided were recorded in the patients’ medical record. Family or significant others were encouraged to join the sessions and were involved in the discussion and information provision.
Training
Six oncology nurses were selected to carry out the intervention. Mean age of the nurses was 44 years (range = 24–59), and mean years working as a nurse was 25 years (range = 10–40), with a mean of 13 years (range = 3–23) as a nurse on the oral maxillofacial and otorhinolaryngology ward.
Preceding the study, the nurses received a three-hour training to increase the skills needed for delivering the intervention in a uniform manner. Where nurses traditionally take a direct approach in solving problems as they are mentioned or occur, training can enable nurses to listen more carefully and to encourage patients and family members to talk about their problems.
The training started with the theoretical background of the DT&PL, followed by practical steps of the procedure. Role playing was used to get familiar with the DT&PL, to practice conversation skills, and to decide when a patient should be referred. The nurses piloted the DT&PL+ intervention with selected patients to test the intervention and to provide feedback. During the study, periodic consultation sessions were organized to discuss difficulties and to ensure that the intervention was offered in a uniform manner under supervision of one of the researchers.
Measures
The primary outcome, depressive symptoms, was measured with the Center for Epidemiologic Studies–Depression scale (CES-D) (Hanewald, 1992; Radloff, 1977). This 20-item self-report questionnaire gives a total score ranging from 0–60 (Bouma, Ranchor, Sanderman, & van Sonderen, 1995). A high score reflects a high level of depression. A cutoff score of 16 or higher is regarded as being indicative of clinical depression. The CES-D has good reliability and validity scores in cancer populations (Beeber, Shea, & McCorkle, 1998; Lewis, Hammond, & Woods, 1993; Pasacreta, 1997), including in patients with HNC (de Graeff et al., 2000; de Leeuw, de Graeff, Ros, Hordijk, et al., 2000; Katz, Irish, Devins, Rodin, & Gullane, 2003). Reliability (Cronbach alpha) is 0.87–0.94.
HRQOL was measured with the European Organisation for Research and Treatment of Cancer (EORTC) Core Quality of Life Questionnaire, version 3.0 (QLQ–C30) (Aaronson et al., 1993) and the tumor-specific EORTC Head and Neck module (QLQ-H&N35) (Bjordal et al., 1999). The QLQ-C30 is widely used and has been validated for many types of cancer, including HNC. Both are widely used and have good reliability validity scores (Bjordal et al., 2000; Singer et al., 2013). Reliability (Cronbach alpha) is 0.61–0.95. The instruments’ scores range from 0–100, where a high score reflects a high level of functioning or a high level of symptoms or problems.
Fear of cancer recurrence was measured with the Worry of Cancer Scale (Easterling & Leventhal, 1989). This questionnaire contains four items scored from 0–10, with a higher score reflecting a higher level of concern. The scale has been validated in patients with breast cancer (Easterling & Leventhal, 1989). Reliability (Cronbach alpha) in the current study was 0.88.
Patient satisfaction with the intervention was measured with nine topics rated on a five-point Likert-type scale from 1 (poor) to 5 (excellent). Each question asked patients to evaluate the nurse in the most recent DT&PL+ sessions relating to willingness to listen to concerns, quality of information, and other topics. The participant could evaluate how satisfied he or she was with the nurse-led sessions on a 1–10 scale. These topics were derived from the EORTC IN-PATSAT32 (Brédart et al., 2005), a questionnaire to measure appraisal of doctors and nurses, and the Consumer Quality Index Cancer Care questionnaire, version 2.0, for measuring experiences with hospital care of patients with different types of care (Booij et al., 2013). Reliability (Cronbach alpha) in the current study was 0.96.
DT&PL outcomes were recorded in the patient record by the nurses who delivered the intervention. The nurses also documented the content of the intervention (i.e., the duration of each appointment, presence of family or significant others, topics discussed, advice and/or intervention given, and referral).
Information was collected about age, gender, educational level, and social status by self-report questionnaires. Information about the type of cancer, tumor stage, and type of treatment was obtained from the medical records.
Sample Size Calculation
The number of patients to be approached was based on the expected change in CES-D scores after one year. In the authors’ previous study (van der Meulen et al., 2013), investigating the effect of a nurse-led psychosocial intervention in patients with HNC, a significant difference (p < 0.05) of 2.9 points (SD = 10) in depressive symptoms was found in favor of the intervention group compared with the control group. This difference corresponds with an effect size of 0.29. Using a two-sided t test with an alpha of 0.05 and a power of 80%, the authors considered a sample size of 144 patients per group to be appropriate.
Because the mixed-models analysis used in the present study was adjusted for baseline CES-D values, the correlation (rho) of 0.54 between the baseline and follow-up CES-D scores found in the previous study (van der Meulen et al., 2013) was taken into account in the sample size calculation. Therefore, the number of participants was multiplied by (1 – rho2), plus one extra patient per group (Borm, Fransen, & Lemmens, 2007), giving a final sample size of 103 patients per group ([1 – 0.542] x 144 + 1), resulting in a total of 206 patients. On the basis of previous studies (de Graeff et al., 1999; van der Meulen et al., 2013), the authors expected that 70% of eligible patients would be included. Therefore, at least 288 patients had to be approached.
Statistical Analysis
The effect of the DT&PL+ intervention was assessed on an intention-to-treat basis using a linear mixed model. The model for the between-group analysis contained depressive symptoms at 6 and 12 months as dependent variables. Measurement and group (intervention versus control) were entered as independent variables, and baseline depressive symptom score was entered as a covariate. All participants who had completed at least the 6- or 12-month assessments were included in the between-group analysis. The model for the within-group analysis followed the same structure; however, no covariate was used and all participants who completed at least the baseline assessment were included. Primary outcomes were the between-group differences at 12 months. Two-sided significant tests were used (p < 0.05). Statistical analyses were performed using IBM SPSS Statistics, version 23.0.
Results
Sample
In six months, 213 patients were invited to participate in the study, of whom 110 (52%) were enrolled. The majority of the 103 patients who declined gave the main reason that they felt no need to participate (n = 39) (see Figure 1). Patients who declined were significantly (p < 0.05) older, more often had TNM staging system classification I–II, and were more often recruited in the first three months after the end of treatment. Included participants had a mean age of 63.5 years (SD = 11.4), were mainly men (75%), and were married or living together (77%). The baseline characteristics of patients in the intervention and control groups were comparable (see Table 1).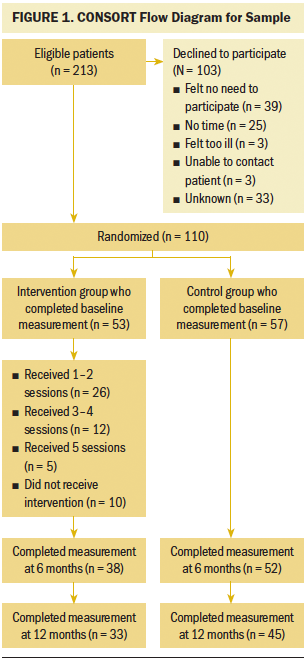
Significant differences (p < 0.05) were found between the 35 (32%) participants who were lost to follow-up and the 75 (68%) participants who completed the study. Participants who were lost to follow-up had a higher level of depressive symptoms, a lower HRQOL, and lower scores on all QLQ-C30 functioning scales at baseline. In addition, these participants had more problems on all QLQ-C30 and QLQ-H&N35 problem scales except for insomnia, loss of appetite, constipation, diarrhea, sexuality, and teeth. They were also more often unemployed and were more often included in the intervention group. During the study period, two participants in the intervention group and four participants in the control group visited a psychologist.
[[{"type":"media","view_mode":"media_original","fid":"38116","attributes":{"alt":"","class":"media-image","height":"955","typeof":"foaf:Image","width":"372"}}]]
Intervention
Of the 53 participants allocated to the intervention group, 26 received 1–2 sessions, 12 received 3–4 sessions, and 5 received 5 sessions. Ten participants received no intervention because of administrative errors (n = 7), failure to show up (n = 2), or severe illness (n = 1).
The mean DT score remained relatively stable over time, with a score of 3.8 at session 1 and 3.7 at session 4. On average, one-third of the participants in the intervention group reported every session as a DT score of 5 or higher. Emotional problems were reported by 40%–60% of participants, most often tension or nervousness. Physical problems were reported by 64%–90% of participants, most often eating and mouth sores, and 24%–41% reported other problems. Of the patients who reported one or more problems, 3%–21% wanted to talk with an expert. More information and details are given in Table 2.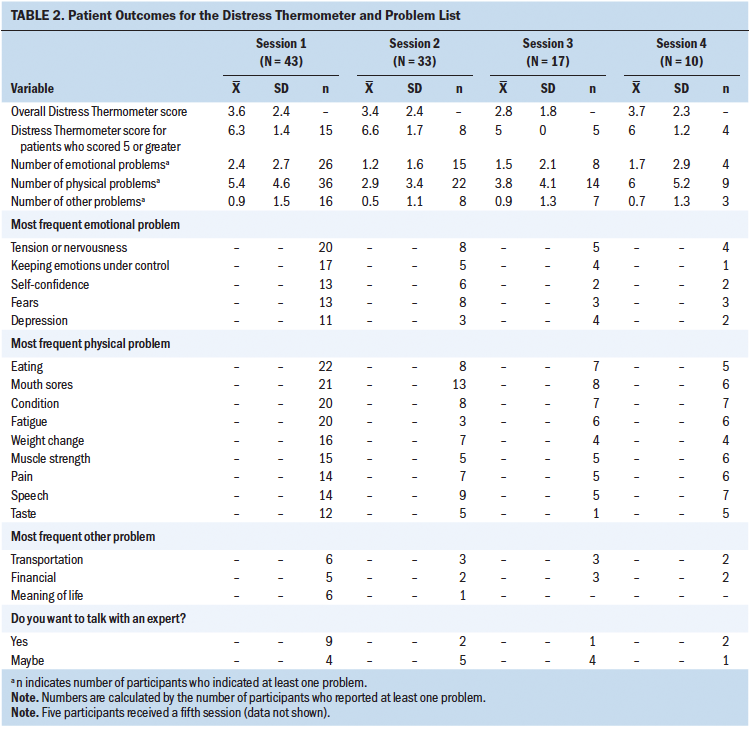
Session 1 took an average of 16.5 minutes, and session 4 took on average 12.2 minutes. Family members or significant others were present in 17%–49% of the sessions. The most discussed topics were physical problems (13%–59%) and family or social problems (3%–41%). Nurses provided information (14%–33%) and gave advice on oral hygiene (8%–17%). Referral to a psychologist (8%) or social worker (3%–17%) was suggested (see Table 3). 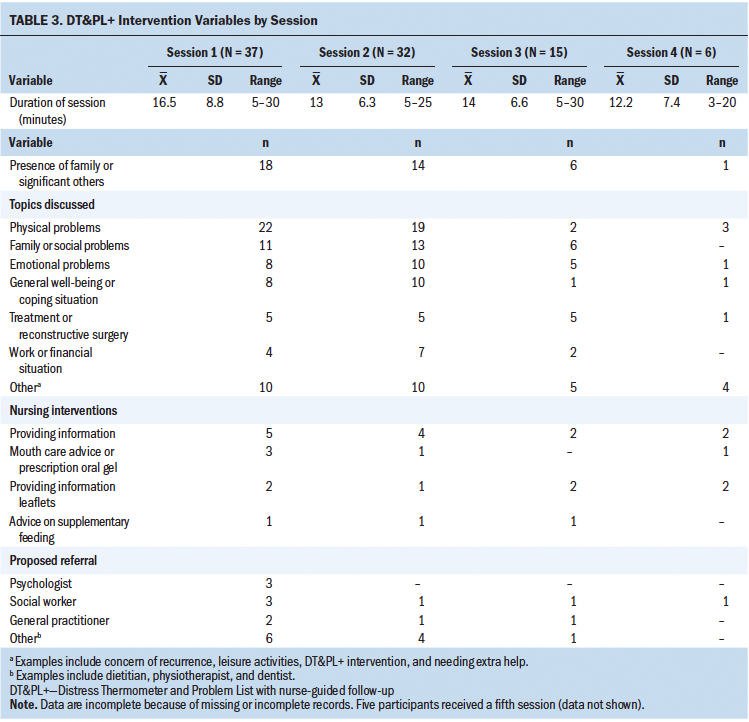
In general, participants in the intervention group were satisfied (scoring good, very good, or excellent) with the nurses’ knowledge; attention paid to physical, emotional, and social problems; personal attention; support and information received; human qualities; and duration of the conversation. On average, the nurses received (on a 1–10 scale) a score of 7.9 (SD = 2.2) and 7.6 (SD = 1.6) at M2 and M3, respectively.
Group Comparisons
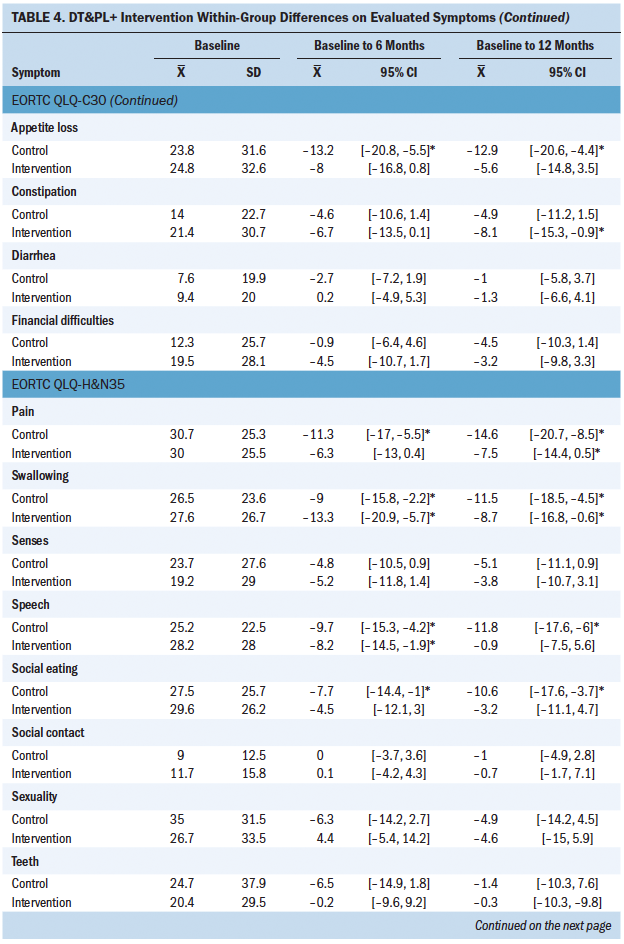
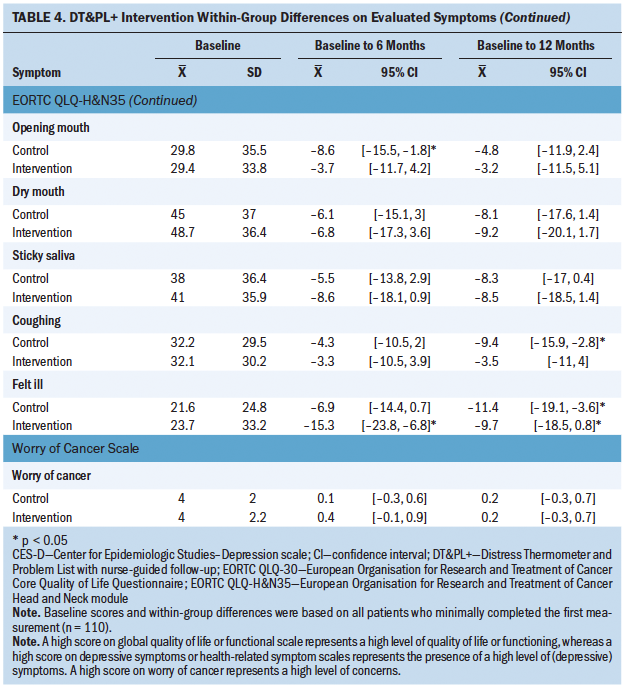
In general, no significant between-group differences were found in depressive symptoms at 6 and 12 months (see Tables 4 and 5). Of all the QLQ-C30 and QLQ-H&N35 items, the variable pain at 6 months and speech at 12 months showed a significant difference between groups in favor of the control group (mean = 10.2, 95% confidence interval [CI] [0.9, 19.5], effect size [ES] = 0.4; mean = 11.3, 95% CI [3.5, 19.1], ES = 0.55, respectively). Although the pain score remained at the same level in the intervention group (mean = –0.7, 95% CI [–8.4, 6.9]), it decreased in the control group (mean = –9.7, 95% CI [–16.5, –3]). Likewise, the speech score in the intervention group remained the same (mean = –0.9, 95% CI [–7.5, 5.6]) and decreased in the control group (mean = –11.8, 95% CI [–17.6, –6]). No significant between-group differences were found with regard to worry about cancer at both time points.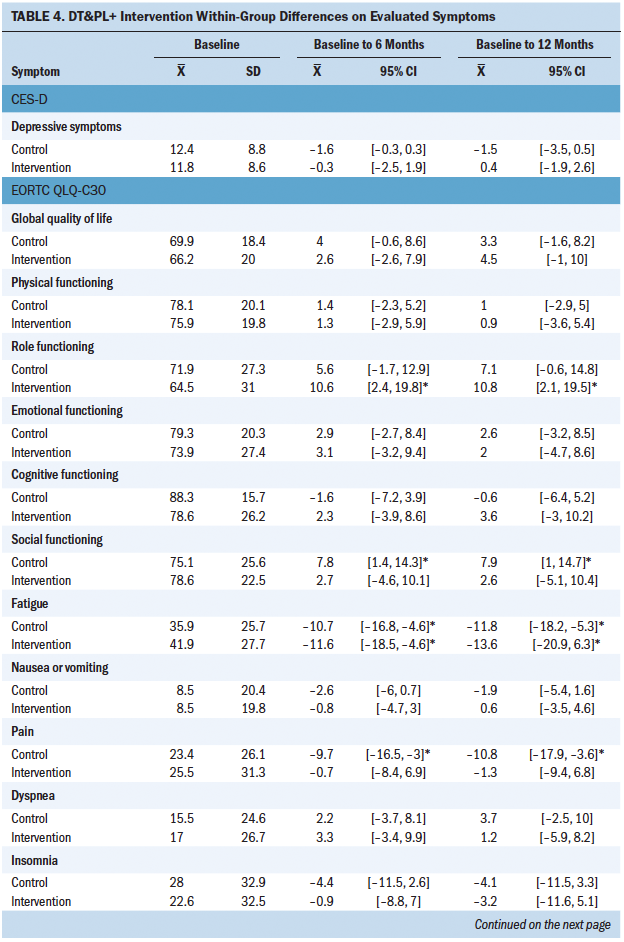
Discussion
This study investigated the effect of the DT&PL+ intervention on depressive symptoms, HRQOL, and worry about cancer in patients with HNC in a randomized, controlled trial. No beneficial effects of the intervention on depressive symptoms, HRQOL, or worry about cancer at 6 or 12 months after inclusion could be shown. About one-third of the participants in the intervention group had raised levels of distress (DT score of 5 or greater), and most participants reported at least one emotional or physical problem. The intervention showed moderate compliance and acceptable session duration. Intervention participants were satisfied with nurses’ care.
This is one of the few studies to assess the effectiveness of the DT&PL+ intervention on patient outcomes during one year (Carlson et al., 2012; Hollingworth et al., 2013) and the first to include only patients with HNC. The nurses who delivered the intervention were experienced in the care of patients with HNC and had received training with follow-up consultation sessions to increase the quality of the intervention and to positively influence patient outcomes (Mitchell, 2013).
[[{"type":"media","view_mode":"media_original","fid":"38121","attributes":{"alt":"","class":"media-image","height":"939","typeof":"foaf:Image","width":"624"}}]]
[[{"type":"media","view_mode":"media_original","fid":"38126","attributes":{"alt":"","class":"media-image","height":"939","typeof":"foaf:Image","width":"624"}}]]
[[{"type":"media","view_mode":"media_original","fid":"38131","attributes":{"alt":"","class":"media-image","height":"686","typeof":"foaf:Image","width":"623"}}]]
As outlined in the review by Fitch (2011), multiple challenges exist to successfully implementing an intervention and to improving patient outcomes. Although several strategies were used to ensure that the study ran smoothly, such as training of staff, engaging stakeholders, and providing feedback audits, the busy day-to-day reality was that the intervention was sometime delayed. The DT&PL+ intervention seems feasible in terms of integration in standard care, duration of sessions, and patient satisfaction, but several practical difficulties concerning the scheduling of sessions and the reporting of sessions need to be improved to achieve optimal implementation.
Although the nurse-led sessions were scheduled directly after the medical check-up, 40% of the participants in the intervention group were lost to follow-up, some because of planning difficulties and some because participants said that they did not feel the need to continue. Perhaps the intervention format did not fit patients’ expectations and desires, or the appointment with the nurse was felt to be an extra burden. The participants who dropped out reported, on average, more depressive symptoms and lower HRQOL scores at baseline. This is in line with the findings of Hollingworth et al. (2013), who reported that participants with better scores at baseline benefitted more from a DT&PL intervention than patients with worse scores at baseline in a group of patients with cancer. Patients with severe problems may need a more structured, intensive intervention. In two of the authors’ previous studies (van der Meulen et al., 2013, 2014), results showed that an intervention consisting of six 45- to 60-minute counseling sessions given by trained nurses in the outpatient clinic had a significant beneficial effect on depressive symptoms of patients with HNC. This intervention was problem-focused and started with a short screening with the Hospital Anxiety and Depression Scale (Zigmond & Snaith, 1983), followed by discussion of current problems and giving advice, emotional support, education, and behavioral training. Patients with cancer who had raised depressive symptom scores (greater than 12 on the CES-D) at baseline particularly benefited from the intervention. More effective interventions were revealed in a review that showed interventions, such as physical exercise interventions, cognitive behavioral therapy, and complementary therapy, were effective in reducing distress in patients with cancer (Yeh, Chung, Hsu, & Hsu, 2014). However, the review included mainly studies of patients with breast cancer, which makes the interpretation and generalization of findings to patients with HNC difficult. Patients with HNC are, on average, older and less educated and have a higher consumption of tobacco and alcohol.
The patients with HNC in the current study often indicated that, if referral was discussed, they did not want to be referred to a psychologist or psychiatrist. Little is known about referral rates or the wishes of patients with HNC. Verdonck-de Leeuw et al. (2009) reported a referral rate of 21%; however, it is not known how many patients actually received psychological care. Research showed that only 28% of referred patients with cancer accepted the referral (Bauwens et al., 2014). Referral rates to a psychologist or social worker in the current study varied from 3%–17%. Because referral rates and acceptance are low, a structured nurse-led intervention integrated into standard aftercare seems to be a promising way to meet patients’ needs. Evidently, referral for those in need remains a component of that aftercare.
Limitations
The current study had some limitations. Fewer patients than estimated participated in the study; instead of the expected 70%, only 50% of the eligible patients were willing to participate. Because of the preplanned implementation of the DT&PL+ intervention as standard care, extending the inclusion period was not possible. In addition, 40% of the participants were lost to follow-up, which resulted in reduced statistical power. Thirty-eight percent of the patients who declined participation felt no need to participate. Patients were invited by their physician at the end of an appointment in the outpatient clinic. Perhaps time was too short to thoroughly inform the patient and emphasize the importance of the study. However, considering the small differences in outcomes between the intervention and control groups, a larger sample size would presumably not change the overall conclusion. In general, the participants in the intervention group reported relatively few complaints, and the overall mean distress score was 3.4; a score of 5 or greater indicated elevated distress. As a consequence, only a minority of patients were in need of additional care or referral. This makes it more difficult to detect any intervention effect. The study sample included mainly men older than age 60 years, which is similar to the Dutch patients with HNC population, but the generalizability of the findings could be limited for other regions. In addition, the feasibility of the intervention could differ in other healthcare settings where a different follow-up system applies.
Implications for Practice
Nurses played a crucial role in delivering the DT&PL+ intervention by leading the conversation and in coordinating care. The patients with HNC were highly satisfied with this nursing aftercare and appreciated the possibility to discuss their problems and challenges with the nurses. However, the DT&PL+ intervention did not reduce depressive symptoms or worry of cancer recurrence, or improve HRQOL. The emphasis on screening and referral with basic psychosocial care and minor interventions does not seem sufficient for patients with HNC. Extending the intervention with directly provided and more comprehensive nursing interventions seems to be needed.
Because the quality of the intervention can influence patient outcomes (Horner, 2012), it is important to organize training and monitor the intervention delivery. Nurses give content to the intervention by making decisions about which questions they ask, which information they provide, to which healthcare professional they refer patients, and which intervention to start. This should be done in a consistent and approved manner.
During the study, there were no signs that patients felt stigmatized by attending the nurse-led intervention, which might have had a positive influence on the acceptance and adherence of the intervention. This was strengthened by the integration of care in the medical follow-up, the continuity of care patients received from the nurses, and the focus on physical and psychosocial problems. These elements should be retained in further development of the intervention.
In addition, the participating nurses enjoyed providing the intervention, felt their nursing profession to be broadened, and appreciated that they could continue patient care after completion of cancer treatment.
Implications for Research
Further research is needed to identify patient subgroups that would benefit the most from the intervention. Therefore, large-scale studies are needed to ensure sufficient power for subgroup analysis. The involvement of family or significant others, as occurred in this study, is important because they also suffer from distress (Balfe et al., 2016). In addition, their support is important to the recovery of patients (Taneja, 2013). Future studies should pay explicit attention to family or significant others in the implementation and evaluation of a DT&PL+ intervention.
Conclusion
The DT&PL+ intervention seems feasible in clinical practice, but more attention needs to be paid to the optimal scheduling of sessions and patient follow-up. Participants in the intervention group were highly satisfied with nurses’ care; however, no positive intervention effects on depressive symptoms, HRQOL, and worry about cancer in patients with HNC were found. More research is needed to investigate interventions of different intensity to be able to offer patients with HNC tailored interventions that meet their psychosocial needs.
About the Author(s)
Ingeborg C. van der Meulen, PhD, RN, is a lecturer in the School of Nursing at Hanzehogeschool Groningen; and Anne M. May, PhD, is an associate professor in the Department of Epidemiology of the Julius Center; Ron Koole, Prof.(em)Dr., was, at the time of writing, a surgeon in the Department of Oral Maxillofacial Surgery; and Wynand J.G. Ros, PhD, is an associate professor in the Department of Public Health, Health Technology Assessment and Medical Humanities of the Julius Center, all at the University Medical Center Utrecht, all in the Netherlands. van der Meulen and Ros contributed to the conceptualization and design and completed the data collection. van der Meulen, May, and Ros provided statistical support and the analysis. All authors contributed to the manuscript preparation. This research was funded by a grant from the Dutch Cancer Society and a grant from the oral maxillofacial clinic at the University Medical Center Utrecht. van der Meulen can be reached at i.c.van.der.meulen@pl.hanze.nl, with copy to ONFEditor@ons.org. (Submitted January 2017. Accepted for publication July 19, 2017.)
References
Aaronson, N.K., Ahmedzai, S., Bergman, B., Bullinger, M., Cull, A., Duez, N.J., . . . de Haes, J.C. (1993). The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. Journal of the National Cancer Institute, 85, 365–376.
Ahn, M.H., Park, S., Lee, H.B., Ramsey, C.M., Na, R., Kim, S.O., . . . Hong, J.P. (2015). Suicide in cancer patients within the first year of diagnosis. Psycho-Oncology, 24, 601–607. https://doi.org/10.1002/pon.3705
Balfe, M., Maguire, R., Hanly, P., Butow, P., O’Sullivan, E., Timmons, A., . . . Sharp, L. (2016). Distress in long-term head and neck cancer carers: A qualitative study of carers’ perspectives. Journal of Clinical Nursing, 25, 2317–2327. https://doi.org/10.1111/jocn.13242
Bauwens, S., Baillon, C., Distelmans, W., & Theuns, P. (2014). Systematic screening for distress in oncology practice using the distress barometer: The impact on referrals to psychosocial care. Psycho-Oncology, 23, 804–811. https://doi.org/10.1002/pon.3484
Beeber, L.S., Shea, J., & McCorkle, R. (1998). TheCenter forEpidemiologic Studies Depression Scale as a measure of depressive symptoms in newly diagnosed patients. Journal of Psychosocial Oncology, 16, 1–20. https://doi.org/10.1300/J077V16N01_01
Bjordal, K., de Graeff, A., Fayers, P.M., Hammerlid, E., van Pottelsberghe, C., Curran, D., . . . Kaasa, S. (2000). A 12 country field study of the EORTC QLQ-C30 (version 3.0) and the head and neck cancer specific module (EORTC QLQ-H&N35) in head and neck patients. European Journal of Cancer, 36, 1796–1807. https://doi.org/10.1016/S0959-8049(00)00186-6
Bjordal, K., Hammerlid, E., Ahlner-Elmqvist, M., de Graeff, A., Boysen, M., Evensen, J.F., . . . Kaasa, S. (1999). Quality of life in head and neck cancer patients: Validation of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire—H&N35. Journal of Clinical Oncology, 17, 1008–1019. https://doi.org/10.1200/JCO.1999.17.3.1008
Booij, J.C., Zegers, M., Evers, P.M., Hendriks, M., Delnoij, D.M., & Rademakers, J.J. (2013). Improving cancer patient care: Development of a generic Cancer Consumer Quality Index Questionnaire for cancer patients. BMC Cancer, 13, 203. https://doi.org/10.1186/1471-2407-13-203
Borm, G.F., Fransen, J., & Lemmens, W.A. (2007). A simple sample size formula for analysis of covariance in randomized clinical trials. Journal of Clinical Epidemiology, 60, 1234–1238. https://doi.org/10.1016/j.jclinepi.2007.02.006
Bornbaum, C.C., Fung, K., Franklin, J.H., Nichols, A., Yoo, J., & Doyle, P.C. (2012). A descriptive analysis of the relationship between quality of life and distress in individuals with head and neck cancer. Supportive Care in Cancer, 20, 2157–2165. https://doi.org/10.1007/s00520-011-1326-2
Bouma, J., Ranchor, A.V., Sanderman, R., & van Sonderen, F.L.P. (1995). Measuring symptoms of depression with the CES-D: A manual [In Dutch]. Groningen, Netherlands: Northern Centre for Healthcare Research, University of Groningen.
Braeken, A.P., Lechner, L., Eekers, D.B., Houben, R.M., van Gils, F.C., Ambergen, T., & Kempen, G.I. (2013). Does routine psychosocial screening improve referral to psychosocial care providers and patient-radiotherapist communication? A cluster randomized controlled trial. Patient Education and Counseling, 93, 289–297. https://doi.org/10.1016/j.pec.2013.06.015
Brédart, A., Bottomley, A., Blazeby, J.M., Conroy, T., Coens, C., D’Haese, S., . . . Aaronson, N.K. (2005). An international prospective study of the EORTC Cancer Inpatient Satisfaction with Care measure (EORTC IN-PATSAT32). European Journal of Cancer, 41, 2120–2131. https://doi.org/10.1016/j.ejca.2005.04.041
Buchmann, L., Conlee, J., Hunt, J., Agarwal, J., & White, S. (2013). Psychosocial distress is prevalent in head and neck cancer patients. Laryngoscope, 123, 1424–1429. https://doi.org/10.1002/lary.23886
Carlson, L.E., Waller, A., Groff, S.L., Zhong, L., & Bultz, B.D. (2012). Online screening for distress, the 6th vital sign, in newly diagnosed oncology outpatients: Randomised controlled trial of computerised vs personalised triage. British Journal of Cancer, 107, 617–625. https://doi.org/10.1038/bjc.2012.309
Carlson, L.E., Waller, A., & Mitchell, A.J. (2012). Screening for distress and unmet needs in patients with cancer: Review and recommendations. Journal of Clinical Oncology, 30, 1160–1177. https://doi.org/10.1200/JCO.2011.39.5509
de Graeff, A., de Leeuw, R.J., Ros, W.J., Hordijk, G.J., Battermann, J.J., Blijham, G.H., & Winnubst, J.A. (1999). A prospective study on quality of life of laryngeal cancer patients treated with radiotherapy. Head and Neck, 21, 291–296.
de Graeff, A., de Leeuw, J.R., Ros, W.J., Hordijk, G., Blijham, G.H., & Winnubst, J.A. (2000). Long-term quality of life of patients with head and neck cancer. Laryngoscope, 110, 98–106. https://doi.org/10.1097/00005537-200001000-00018
de Leeuw, J.R., de Graeff, A., Ros, W.J., Blijham, G.H., Hordijk, G.J., & Winnubst, J.A. (2000). Prediction of depressive symptomatology after treatment of head and neck cancer: The influence of pre-treatment physical and depressive symptoms, coping, and social support. Head and Neck, 22, 799–807.
de Leeuw, J.R., de Graeff, A., Ros, W.J., Hordijk, G.J., Blijham, G.H., & Winnubst, J.A. (2000). Negative and positive influences of social support on depression in patients with head and neck cancer: A prospective study. Psycho-Oncology, 9, 20–28.
Donovan, K.A., Grassi, L., McGinty, H.L., & Jacobsen, P.B. (2014). Validation of the Distress Thermometer worldwide: State of the science. Psycho-Oncology, 23, 241–250. https://doi.org/10.1002/pon.3430
Dunne, S., Mooney, O., Coffey, L., Sharp, L., Desmond, D., Timon, C., . . . Gallagher, P. (2017). Psychological variables associated with quality of life following primary treatment for head and neck cancer: A systematic review of the literature from 2004 to 2015. Psycho-Oncology, 26, 149–160. https://doi.org/10.1002/pon.4109
Easterling, D.V., & Leventhal, H. (1989). Contribution of concrete cognition to emotion: Neutral symptoms as elicitors of worry about cancer. Journal of Applied Psychology, 74, 787–796.
Fitch, M.I. (2011). Screening for distress: A role for oncology nursing. Current Opinion in Oncology, 23, 331–337. https://doi.org/10.1097/CCO.0b013e32834791a1
Ghazali, N., Roe, B., Lowe, D., Tandon, S., Jones, T., Brown, J., . . . Rogers, S.N. (2017). Screening for distress using the Distress Thermometer and the University of Washington quality of life in post-treatment head and neck cancer survivors. European Archives of Otorhinolaryngology, 274, 2253–2260. https://doi.org/10.1007/s00405-017-4474-2
Hammerlid, E., Silander, E., Hörnestam, L., & Sullivan, M. (2001). Health-related quality of life three years after diagnosis of head and neck cancer—A longitudinal study. Head and Neck, 23, 113–125.
Hanewald, G.J. (1992). CES-D—The Dutch version: An investigation of reliability and validity. Unpublished manuscript, Department of Clinical Oncology, University of Amsterdam.
Heijnen, B.J., Speyer, R., Kertscher, B., Cordier, R., Koetsenruijter, K.W., Swan, K., & Bogaardt, H. (2016). Dysphagia, speech, voice, and trismus following radiotherapy and/or chemotherapy in patients with head and neck carcinoma: Review of the literature. BioMed Research International, 2016, 6086894. https://doi.org/10.1155/2016/6086894
Hollingworth, W., Metcalfe, C., Mancero, S., Harris, S., Campbell, R., Biddle, L., . . . Brennan, J. (2013). Are needs assessments cost effective in reducing distress among patients with cancer? A randomized controlled trial using the Distress Thermometer and problem list. Journal of Clinical Oncology, 31, 3631–3638. https://doi.org/10.1200/JCO.2012.48.3040
Horner, S.D. (2012). Best practices for improving intervention fidelity that every nurse should know. Journal for Specialists in Pediatric Nursing, 17, 171–174. https://doi.org/10.1111/j.1744-6155.2012.00327.x
Jiang, N., Zhao, Y., Jansson, H., Chen, X., & Mårtensson, J. (2017). Experiences of xerostomia after radiotherapy in patients with head and neck cancer: A qualitative study. Journal of Clinical Nursing. Advance online publication. https://doi.org/10.1111/jocn.13879
Katz, M.R., Irish, J.C., Devins, G.M., Rodin, G.M., & Gullane, P.J. (2003). Psychosocial adjustment in head and neck cancer: The impact of disfigurement, gender and social support. Head and Neck, 25, 103–112. https://doi.org/10.1002/hed.10174
Kissun, D., Magennis, P., Lowe, D., Brown, J.S., Vaughan, E.D., & Rogers, S.N. (2006). Timing and presentation of recurrent oral and oropharyngeal squamous cell carcinoma and awareness in the outpatient clinic. British Journal of Oral and Maxillofacial Surgery, 44, 371–376. doi:10.1016/j.bjoms.2005.08.010
Krebber, A.M., Jansen, F., Cuijpers, P., Leemans, C.R., & Verdonck-de Leeuw, I.M. (2016). Screening for psychological distress in follow-up care to identify head and neck cancer patients with untreated distress. Supportive Care in Cancer, 24, 2541–2548. https://doi.org/10.1007/s00520-015-3053-6
Lester, J., Crosthwaite, K., Stout, R., Jones, R.N., Holloman, C., Shapiro, C., & Andersen, B.L. (2015). Women with breast cancer: Self-reported distress in early survivorship [Online exclusive]. Oncology Nursing Forum, 42, E17–E23. https://doi.org/10.1188/15.ONF.E17-E23
Lewis, F. M., Hammond, M. A., & Woods, N. F. (1993). The family’s functioning with newly diagnosed breast cancer in the mother: The development of an explanatory model. Journal of Behavioral Medicine, 16, 351–370.
Ma, X., Zhang, J., Zhong, W., Shu, C., Wang, F., Wen, J., . . . Liu, L. (2014). The diagnostic role of a short screening tool—The Distress Thermometer: A meta-analysis. Supportive Care in Cancer, 22, 1741–1755. https://doi.org/10.1007/s00520-014-2143-1
Mehanna, H.M., & Morton, R.P. (2006). Deterioration in quality-of-life of late (10-year) survivors of head and neck cancer. Clinical Otolaryngology, 31, 204–211. https://doi.org/10.1111/j.1749-4486.2006.01188.x
Meijer, A., Roseman, M., Delisle, V.C., Milette, K., Levis, B., Syamchandra, A., . . . Thombs, B.D. (2013). Effects of screening for psychological distress on patient outcomes in cancer: A systematic review. Journal of Psychosomatic Research, 75, 1–17. https://doi.org/10.1016/j.jpsychores.2013.01.012
Mitchell, A.J. (2013). Screening for cancer-related distress: When is implementation successful and when is it unsuccessful? Acta Oncologica, 52, 216–224. https://doi.org/10.3109/0284186X.2012.745949
Ninu, M.B., Miccinesi, G., Bulli, F., De Massimi, A., Muraca, M.G., Franchi, G., & Squadrelli Saraceno, M. (2016). Psychological distress and health-related quality of life among head and neck cancer patients during the first year after treatment. Tumori, 102, 96–102. https://doi.org/10.5301/tj.5000448
Oskam, I.M., Verdonck-de Leeuw, I.M., Aaronson, N.K., Witte, B.I., de Bree, R., Doornaert, P., . . . Leemans, C.R. (2013). Prospective evaluation of health-related quality of life in long-term oral and oropharyngeal cancer survivors and the perceived need for supportive care. Oral Oncology, 49, 443–448. https://doi.org/10.1016/j.oraloncology.2012.12.005
Ottosson, S., Laurell, G., & Olsson, C. (2013). The experience of food, eating and meals following radiotherapy for head and neck cancer: A qualitative study. Journal of Clinical Nursing, 22, 1034–1043. https://doi.org/10.1111/jocn.12151
Pandey, M., Devi, N., Ramdas, K., Krishnan, R., & Kumar, V. (2009). Higher distress relates to poor quality of life in patients with head and neck cancer. International Journal of Oral and Maxillofacial Surgery, 38, 955–959. https://doi.org/10.1016/j.ijom.2009.04.004
Pasacreta, J.V. (1997). Depressive phenomena, physical symptom distress, and functional status among women with breast cancer. Nursing Research, 46(4), 214–221.
Petty, L., & Lester, J. (2014). Distress screening in chronic disease: Essential for cancer survivors. Journal of the Advanced Practitioner in Oncology, 5, 107–114.
Ploos van Amstel, F.K., Prins, J.B., van der Graaf, W.T., Peters, M.E., & Ottevanger, P.B. (2016). The effectiveness of a nurse-led intervention with the distress thermometer for patients treated with curative intent for breast cancer: Design of a randomized controlled trial. BMC Cancer, 16, 520. https://doi.org/10.1186/s12885-016-2565-x
Ploos van Amstel, F.K., van den Berg, S.W., van Laarhoven, H.W., Gielissen, M.F., Prins, J.B., & Ottevanger, P.B. (2013). Distress screening remains important during follow-up after primary breast cancer treatment. Supportive Care in Cancer, 21, 2107–2115. https://doi.org/10.1007/s00520-013-1764-0
Radloff, L.S. (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401. https://doi.org/10.1177/014662167700100306
Rinkel, R.N., Verdonck-de Leeuw, I.M., Doornaert, P., Buter, J., de Bree, R., Langendijk, J.A., . . . Leemans, C.R. (2016). Prevalence of swallowing and speech problems in daily life after chemoradiation for head and neck cancer based on cut-off scores of the patient-reported outcome measures SWAL-QOL and SHI. European Archives of Otorhinolaryngology, 273, 1849–1855. https://doi.org/10.1007/s00405-015-3680-z
Rogers, S.N., Ahad, S.A., & Murphy, A.P. (2007). A structured review and theme analysis of papers published on ‘quality of life’ in head and neck cancer: 2000–2005. Oral Oncology, 43, 843–868. https://doi.org/10.1016/j.oraloncology.2007.02.006
Rogers, L.Q., Rao, K., Malone, J., Kandula, P., Ronen, O., Markwell, S.J., . . . Robbins, K.T. (2009). Factors associated with quality of life in outpatients with head and neck cancer 6 months after diagnosis. Head and Neck, 31, 1207–1214. https://doi.org/10.1002/hed.21084
Rogers, S.N., Heseltine, N., Flexen, J., Winstanley, H.R., Cole-Hawkins, H., & Kanatas, A. (2016). Structured review of papers reporting specific functions in patients with cancer of the head and neck: 2006–2013. British Journal of Oral and Maxillofacial Surgery, 54, e45–e51. https://doi.org/10.1016/j.bjoms.2016.02.012
Ronis, D.L., Duffy, S.A., Fowler, K.E., Khan, M.J., & Terrell, J.E. (2008). Changes in quality of life over 1 year in patients with head and neck cancer. Archives of Otolaryngology—Head and Neck Surgery, 134, 241–248. https://doi.org/10.1001/archoto.2007.43
Roth, A.J., Kornblith, A.B., Batel-Copel, L., Peabody, E., Scher, H.I., & Holland, J.C. (1998). Rapid screening for psychologic distress in men with prostate carcinoma: A pilot study. Cancer, 82, 1904–1908.
Semple, C.J., Dunwoody, L., Kernohan, G.W., McCaughan, E., & Sullivan, K. (2008). Changes and challenges to patients’ lifestyle patterns following treatment for head and neck cancer. Journal of Advanced Nursing, 63, 85–93. https://doi.org/10.1111/j.1365-2648.2008.04698.x
Simonelli, L.E., Siegel, S.D., & Duffy, N.M. (2016). Fear of cancer recurrence: A theoretical review and its relevance for clinical presentation and management. Psycho-Oncology. https://doi.org/10.1002/pon.4168
Singer, S., Arraras, J.I., Chie, W.C., Fisher, S.E., Galalae, R., Hammerlid, E., . . . Hofmeister, D. (2013). Performance of the EORTC questionnaire for the assessment of quality of life in head and neck cancer patients EORTC QLQ-H&N35: A methodological review. Quality of Life Research, 22, 1927–1941. https://doi.org/10.1007/s11136-012-0325-1
Singer, S., Krauss, O., Keszte, J., Siegl, G., Papsdorf, K., Severi, E., . . . Kortmann, R.D. (2012). Predictors of emotional distress in patients with head and neck cancer. Head and Neck, 34, 180–187. https://doi.org/10.1002/hed.21702
Snowden, A., White, C.A., Christie, Z., Murray, E., McGowan, C., & Scott, R. (2011). The clinical utility of the Distress Thermometer: A review. British Journal of Nursing, 20, 220–227. https://doi.org/10.12968/bjon.2011.20.4.220
Taneja, M.K. (2013). Life style management in head and neck cancer patients. Indian Journal of Otolaryngology and Head and Neck Surgery, 65, 289–292. https://doi.org/10.1007/s12070-013-0682-2
Tuinman, M.A., Gazendam-Donofrio, S.M., & Hoekstra-Weebers, J.E. (2008). Screening and referral for psychosocial distress in oncologic practice: Use of the Distress Thermometer. Cancer, 113, 870–878. https://doi.org/10.1002/cncr.23622
van der Meulen, I.C., May, A.M., de Leeuw, J.R., Koole, R., Oosterom, M., Hordijk, G.J., & Ros, W.J. (2014). Long-term effect of a nurse-led psychosocial intervention on health-related quality of life in patients with head and neck cancer: A randomised controlled trial. British Journal of Cancer, 110, 593–601. https://doi.org/10.1038/bjc.2013.733
van der Meulen, I.C., May, A.M., Ros, W.J., Oosterom, M., Hordijk, G.J., Koole, R., & de Leeuw, J.R. (2013). One-year effect of a nurse-led psychosocial intervention on depressive symptoms in patients with head and neck cancer: A randomized controlled trial. Oncologist, 18, 336–344. https://doi.org/10.1634/theoncologist.2012-0299
Van Liew, J.R., Christensen, A.J., Howren, M.B., Hynds Karnell, L., & Funk, G.F. (2014). Fear of recurrence impacts health-related quality of life and continued tobacco use in head and neck cancer survivors. Health Psychology, 33, 373–381. https://doi.org/10.1037/a0032680
Verdonck-de Leeuw, I.M., de Bree, R., Keizer, A.L., Houffelaar, T., Cuijpers, P., van der Linden, M.H., & Leemans, C.R. (2009). Computerized prospective screening for high levels of emotional distress in head and neck cancer patients and referral rate to psychosocial care. Oral Oncology, 45(10), e129–e133. https://doi.org/10.1016/j.oraloncology.2009.01.012
Yeh, M.L., Chung, Y.C., Hsu, M.Y., & Hsu, C.C. (2014). Quanti-fying psychological distress among cancer patients in interventions and scales: A systematic review. Current Pain and Headache Reports, 18, 399. https://doi.org/10.1007/s11916-013-0399-7
Zigmond, A.S., & Snaith, R.P. (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica, 67, 361–370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x


