Experiences of Women With Gestational Trophoblastic Neoplasia Treated With High-Dose Chemotherapy and Stem Cell Transplantation: A Qualitative Study
Purpose/Objectives: To explore the experiences of women with gestational trophoblastic neoplasia during and after treatment to understand their perspectives, priorities, and concerns.
Research Approach: A descriptive, exploratory study using in-depth semistructured interviews.
Setting: All interviews were conducted in a quiet, designated room at Weston Park Hospital in Sheffield, South Yorkshire.
Participants: Women with gestational trophoblastic neoplasia who had received stem cell transplantation from 2003 to 2013. Ten patients were eligible, and eight agreed to participate.
Methodologic Approach: Interviews were carried out over the phone and were recorded and transcribed verbatim. Framework analysis was carried out to generate in-depth descriptions of participants’ experiences.
Findings: Participants described significant physical, psychological, and social effects during and following treatment. Recovery was slow, and treatment had long-term effects on sexuality and body image. The impact of the women’s diagnosis and treatment on their children was a primary concern.
Interpretation: The study provided insight into the multidimensional impact of stem cell transplantation, which can continue after treatment. The need for family-centered services for patients with dependent children was identified.
Implications for Nursing: Nurses need to develop services that effectively communicate the challenges of stem cell transplantation to patients and provide family-centered care and late effects and rehabilitation services.
Jump to a section
Women receiving high-dose chemotherapy with stem cell transplantation for gestational trophoblastic neoplasia (GTN) face unique challenges associated with a rare cancer diagnosis that requires arduous treatment and an uncertain outcome. The purpose of the study was to explore the experiences of women with GTN following high-dose chemotherapy with stem cell transplantation to understand their perspectives, priorities, and concerns.
Gestational trophoblastic disease (GTD) comprises a group of pregnancy-related tumors arising from the trophoblastic tissue, one of which is called a hydatidiform mole (complete or partial). The worldwide incidence of GTD varies considerably; in the United Kingdom, the incidence of GTD is about 1.5 per 1,000 live births, and the incidence in the United States is similar (Choi, Lee, Smith, & Kim, 2015). In most cases, GTD presents as a benign tumor, but malignant change occurs in about 15% of complete moles and in 0.5%–1% of partial moles (Choi et al., 2015). The onset of malignant change is termed gestational trophoblastic neoplasia (GTN) and encompasses a spectrum of tumors, including invasive moles, choriocarcinomas, placenta site trophoblastictumors, and epithelioid trophoblastic tumors (Seckl, Sebire, & Berkowitz, 2010). About 1,550 women are registered and monitored for GTD, and about 135 are treated with GTN annually in the United Kingdom (Tidy, 2016).
GTN is curable with chemotherapy in most women, despite the presence of widespread metastases (Sarwar, Newlands, & Seckl, 2004). Most patients have complete response with monochemotherapy, such as methotrexate (Trexall®) and dactinomycin (Cosmegen®) (Lok, Singh, Fisher, Hancock, & Seckl, 2015). However, an estimated 20%–25% of women with high-risk GTN will have incomplete response to conventional chemotherapy or will relapse from remission (Alazzam et al., 2012; El-Helw et al., 2005). These resistant cancers require further treatment, such as high-dose chemotherapy with stem cell transplantation with curative intent (Lok et al., 2015). The use of this treatment for GTN is increasing, being introduced earlier in the process for those with extensive disease.
According to Wenzel et al. (2002), fear of the unknown and disease recurrence are stress factors that influence the quality of life in patients with GTN. Those requiring stem cell transplantation have high-risk advanced disease; many have not responded to previous chemotherapy or have relapsed following treatment, which may influence their experience during and after treatment. High-dose chemotherapy with stem cell transplantation is associated with significant immediate and long-term physical and psychosocial morbidity, potential mortality, and slow recovery (Bird et al., 2010; Mosher, Redd, Rini, Burkhalter, & DuHamel, 2009; Wu et al., 2011). Although high-dose chemotherapy can be used to treat a range of cancers, it is more widely used in hematology/oncology (Adelstein, Anderson, & Taylor, 2014), and research has tended to focus on patients with hematologic cancers. Little is known about the experiences and concerns of women with GTN receiving this treatment.
GTN is a pregnancy-related malignancy, and many patients are diagnosed and treated while they are caring for children at home. Previous studies exploring the impact of cancer and its treatment on parenting have identified that women in this situation can struggle to balance the physical and emotional demands of their illness and treatment with the demands of parenting and meeting their children’s needs for care (Arès, Lebel, & Bielajew, 2014; Fisher & O’Connor, 2012). Minimizing the disruption brought on by cancer and treatment by maintaining routines and trying to create a sense of normalcy have been identified as important aims of parents with cancer (Semple & McCance, 2010; Strickland, Wells, & Porr, 2015). Meeting these aims can be particularly difficult for women with GTN because of the way treatment and services are delivered.
In the United Kingdom, GTN services have been centralized to two specialist centers, Weston Park Hospital in South Yorkshire and Charing Cross Hospital in London, to optimize effective treatment delivery for this rare cancer (Froeling & Seckl, 2014). Many patients have to travel some distance for treatment, which can include inpatient stays for longer chemotherapy regimens. The potential for disruption is heightened with stem cell transplantations because two cycles are given, each requiring an in-patient hospital stay for as many as four weeks. It also entails a period of protective isolation related to prolonged neutropenic episodes. The thoughts and feelings of women with GTN about stem cell transplantation, including separation from home and family, have not been explored; little is known about the priorities and concerns of these patients. Exploring this subject will provide an opportunity to gain additional insight into the impact of stem cell transplantation on parents who have dependent children living at home.
Healthcare professionals should understand the concerns and priorities of women with GTN to meet their needs. This study aims to provide insight into their experiences.
Methods
A descriptive qualitative methodology was adopted, using semistructured telephone interviews, to explore the personal perspectives and experiences of patients with GTN receiving high-dose chemotherapy and stem cell transplantation.
Sample and Setting
Participants were recruited from all surviving patients who had received high-dose chemotherapy for GTN and had been treated at one of the two treatment centers in the United Kingdom from 2003 to 2013. Twenty-one women with GTN had received this treatment during this period, and 10 were still living at the time of the study. GTN nurses from each center identified potential participants from a registry database for GTD that is maintained by the specialist centers. Each patient was contacted by the nurse specialist for the GTN service at each center and was informed about the study and the consent process. Patients who expressed an interest were sent written information about the study by mail, along with consent forms and contact numbers for additional information. Potential participants were given four weeks to return consent forms; if they did not return the forms, the chief investigator contacted them to ensure they had received the information and to answer any questions. Those who returned consent forms were then contacted by the primary investigator to schedule the interviews and were sent the interview schedule by mail or email. The 10 surviving patients were invited to be interviewed, and 8 agreed to participate in the study. 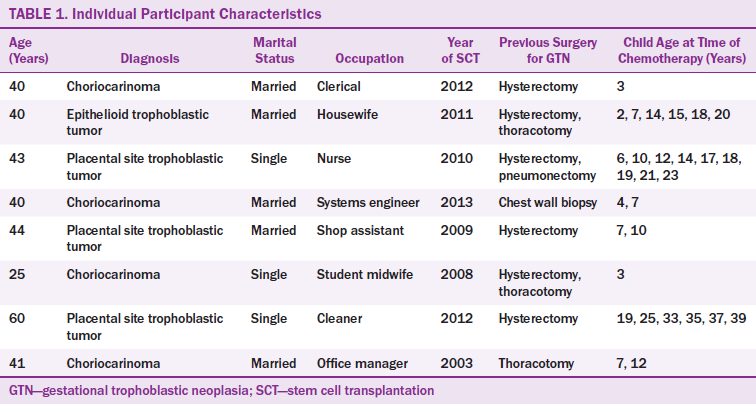
The relatively small sample in the current study reflects the number of surviving patients with GTN who had received stem cell transplantations in the United Kingdom at the time of the interviews. However, the sample was sufficient to secure a range of perspectives and views and achieve an in-depth understanding of patients’ experiences.
Participant demographic information, which was obtained from the registry database and patient case notes (sent with their consent), is detailed in Table 1. One participant did not speak English, so a telephone interpreter service was used. All participants were disease free and not receiving treatment for GTN at the time of the initial interview. One patient subsequently relapsed after the initial interview.
Data Collection
A semistructured interview guide (see Figure 1) was developed, representing the aims of the study following consultation with the GTN specialist nursing teams from both centers. The questions were open-ended with prompts providing structure, allowing participants to provide detailed information about their experiences. The questionnaire was not piloted, but, as the study progressed, additional prompts were introduced to follow lines of inquiry that had emerged in earlier interviews.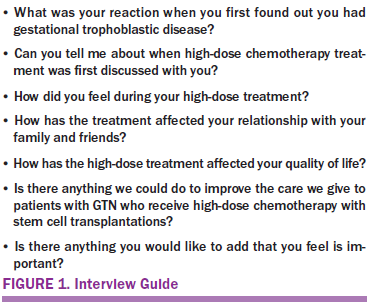
The eight interviews were conducted from September–November 2014 by a member of the project team who had not been involved in the care of patients with GTN. This team member is an experienced oncology nurse and qualitative researcher with expertise in conducting and analyzing interviews with patients regarding their experiences of cancer and treatments. The duration of each interview ranged from 44–107 minutes, and they were conducted by telephone from one of the specialist centers in a private, designated room.
Data Analysis
The interviews were digitally recorded and transcribed verbatim, and the transcripts were checked for accuracy by the chief investigator. Interviews were analyzed using framework analysis, a systematic and transparent process that involves the stages of familiarization, identification of themes, indexing, charting, mapping, and interpretation (Ritchie, Lewis, Nicholls, & Ormston, 2013). Familiarization with transcribed interviews was gained by reading through them multiple times. Themes were identified for initial thematic framework, and content identified in the transcripts in relation to each theme was charted into the framework under the thematic categories. Attributes and characteristics of each theme and the relationships between them were identified and mapped, and descriptive and explanatory accounts of themes were developed. To enhance the reliability of the study, each stage of the analytic process was carried out by two investigators independently, who then met to discuss their findings and reach agreement before progressing to the next stage.
Following first-stage data analysis, all participants were contacted for a follow-up telephone interview to verify and discuss the preliminary findings. A summary of the findings was sent to all participants, who were given four weeks to contact the chief investigator to arrange another interview if they wished to participate. Four participants agreed to be interviewed; of those who declined, one had moved to a different country and three expressed an interest but did not reply to the interview request. These interviews were also recorded and transcribed, and the data were incorporated into the analysis. Final thematic framework and explanatory accounts were agreed on by the investigators. All necessary national and local ethical approvals from the Sheffield Teaching Hospital, Imperial College Healthcare and National Research Ethics Service Committee London-City and East, and the London Health Research Authority were received.
Findings
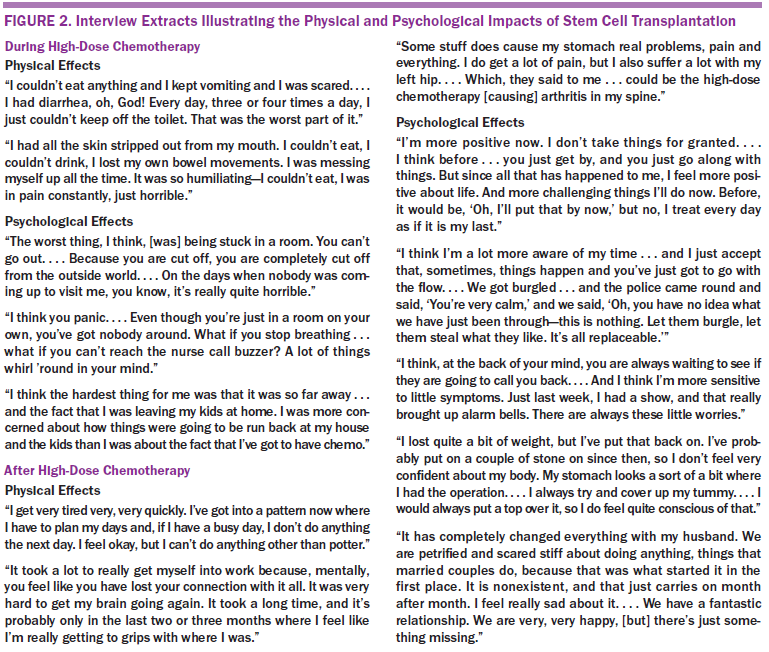
Two core themes were identified. The first related to participants’ descriptions of the physical and psychological impact of treatment. The second represented factors that emerged as priority concerns for participants across the interviews—the implications of GTN and its treatment on their children, their family, and others close to them. Descriptions of the thematic findings are presented sequentially in the following sections. Additional extracts are presented in Figures 2 and 3.
Physical and Psychological Impacts of Treatment
During chemotherapy and stem cell transplantation: Physical side effects were experienced by all participants during treatment. The most common side effects included severe diarrhea, nausea, vomiting, extreme fatigue, sore mouth, and inability to eat or drink. In addition to physical effects, negative thoughts and feelings, such as fear, panic, and worry about dying from the treatment or infection, were mentioned. Being alone was described as one of the most difficult aspects of treatment, partly because few distractions from worrisome thoughts existed and partly because of the frightening thought that no one would notice if they became unwell. The words patients used to describe their experiences, although time had passed since their treatment, provided insight into how significant and distressing their experiences were.
Physically, it was horrible. I was just having diarrhea all the time, literally just standing up and it pouring out. . . . I felt really sick, and I just had no energy whatsoever . . . but then the fear, just lying there on my own for so long and worrying about what might happen. I don’t think it can be described. It’s impossible to describe.
Being away from home and separated from children was a particularly difficult aspect of treatment for many.
Inside, I was hurting a lot. I just wanted to go home to my children. Even though I knew I was in the best place, there is nothing like your family, just to see them and make sure that they are all right.
All participants described how they had been fully informed about the significant risks and side effects associated with stem cell transplantation. However, despite feeling well-informed beforehand, some reported that it was worse than they had expected: “I knew it was going to be difficult, but, until I was in it, I didn’t realize how tough.”
After stem cell transplantation: Recovery emerged as an important theme in descriptions of the post-treatment phase. It was described as a slow, difficult process that occurred over a prolonged period, particularly with longer-lasting side effects, such as tiredness and weakness. Many reported physical effects that were still a problem at the time of the interview, including nerve damage, particularly in the fingers and feet; hearing loss; breathing problems; fatigue that affected daily living; digestive issues; and impaired concentration.
Overall, the participants spoke positively about their current situation and recovery from treatment. Some described how their experiences had helped them find new priorities in life and had given them a sense of their own strength and ability to cope.
It has definitely made me think. I have always been a bit of a worrier, and now I don’t worry about silly things anymore. I look at the big picture. It has definitely made me a stronger person.
Alongside this positive potential, treatment also had negative long-term psychological effects, including anxiety about GTN coming back. These fears had grown less with time but easily could return, particularly at the time of tests, receiving results, or experiencing symptoms that could be interpreted as recurrence.
When you are having treatment, you know that something is being done and then when you go on to being monitored. . . . My life was on hold because I was waiting for something to happen and that I would have to go back and have more treatment. It took awhile to stop thinking like that.
Some participants had lost confidence in their body image because of changes brought on by treatment, such as surgical scars and weight gain. Some felt less interested in sex, partly because of the way they felt about their body but also because they had less desire to engage in sexual activity. These changes had a negative impact on the sexual relationships of participants during treatment and, for some, was still a concern at the time of the interview.
I just don’t have that desire. I care deeply and love him and don’t want to be with anyone else, but my sexual desire is very much diminished from [the treatment]. It’s a combination of how I feel physically about myself and I’m out of the habit, I guess.
Impact on Family Members
All participants were concerned about the effect of their cancer and treatment on their children. Some of the children were worried and anxious about being separated from them during treatment, knowing they had cancer, and/or seeing them unwell with side effects. Some described how their children had been affected emotionally, becoming more needy, clingy, or emotional. Those with school-age children also worried about their children’s education and experience at school.
It did affect them, because they were just emotional all the time. Even in high school, my children were finding it hard to study. My last little lad . . . has just gone to high school, so hopefully it will be the starting point of something new for him.
Not being there for their children during treatment was a source of significant worry. Many recalled measures they had taken so they could be confident their children were well looked after and so they had some stability when they were absent because of treatment. This frequently involved handing over the caregiving role to female family members, such as mothers or older daughters. Some women also described their fears of dying and not being there for their children in the future, which was a source of anxiety but also a reason to undergo the treatment and survive.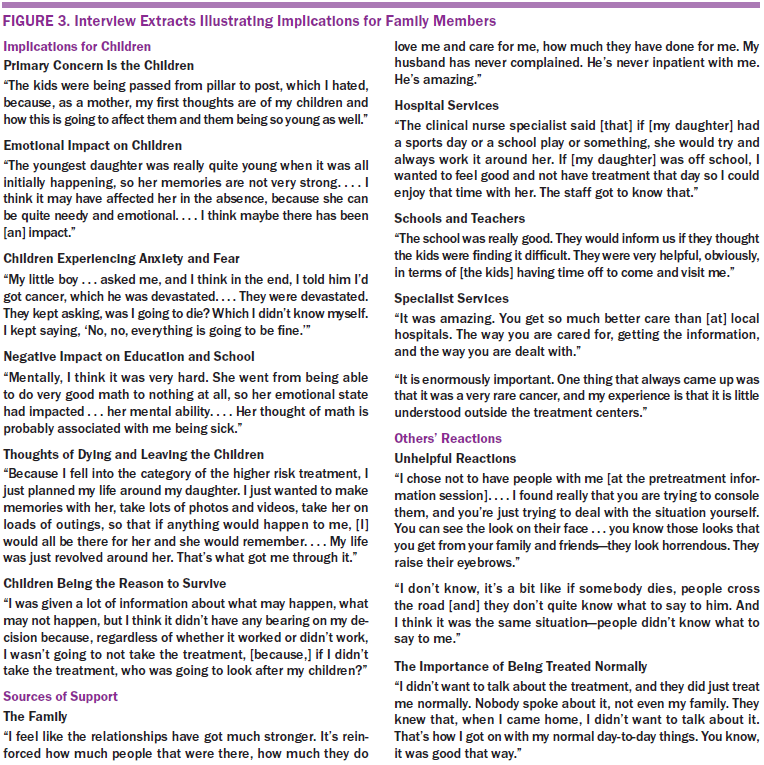
The children were young, so it had a flip side. You [knew] it was horrible because your children were so young.
Influences that were described as helpful in meeting these concerns were practical and psychological support from partners, family, and friends; healthcare services that recognized the importance of parenting responsibilities and tried to be flexible with them; and teachers who understood their situation. A mix of positive and negative experiences of reactions from others were recalled. Unhelpful behaviors and attitudes included not being treated as normal and being too emotional or sympathetic. Participants also described the importance of others recognizing and trying to understand their challenges.
The need for this balanced approach to support extended to their partners. Providing support in a helpful way was identified as a real source of strength. However, not all were able to do this: “My husband was awful—he put his head in the sand—he decided that, as soon as I came home, I was normal, but you’re not.”
Specialist GTN services were praised, and some recounted negative experiences at local hospitals because of healthcare professionals’ lack of knowledge about GTN and its treatment. Trust was built through ongoing relationships with staff members and confidence in their knowledge.
You feel visible and not just a number. They know you. When you ring up, you can pick up where you left off. . . . It was a really difficult time in my life, and my emotions and reactions [were] all over the place. . . . I have given some of them a hard time, but, if I was not familiar with the nurses, I would not be able to do that.
Discussion
The current study, which complements a clinical study of the same patients (Lok et al., 2015), provided valuable insight into the experiences of women with GTN who received stem cell transplantation. The physical challenges described by the participants were similar to those identified in the literature (Adelstein et al., 2014; Bird et al., 2010). The ways in which they described their experiences years after the stem cell transplantation revealed the intensity and duration of their impact.
Treatment was described as difficult, frightening, and highly unpleasant because of a range of physical, psychological, and social factors. Although participants reported feeling well-informed beforehand, some thought treatment was worse than they had expected, suggesting a possible gap between the information they were provided with and their experiences. The current study did not evaluate the content of the information patients were given, which may have reflected the priorities and perspectives of healthcare staff, which may differ from those of patients. Accurate information that prepares patients has been shown to play a role in reducing fear and anxiety during and after treatment (Sutherland, Dpsych, White, Jefford, & Hegarty, 2008). How to best achieve this warrants further investigation. One consideration is to use past experiences of patients, such as those gathered in this study, to develop information that reflects the perspectives of those receiving treatment.
The women’s concerns about their children’s welfare was significant. The separation necessitated by treatment was described as difficult and painful. Studies have identified that women with cancer who have dependent children at home struggle to meet the dual challenges of being a mother and being a patient (Semple & McCance, 2010). This challenge can be heightened if healthcare services focus on the cancer and its treatment without considering their impact on parenting roles and responsibilities (Fisher & O’Connor, 2012).
Maintaining normalcy, establishing routines, and ensuring that their children were well-looked after in their absence have been identified as concerns of women with cancer and dependent children (Elmberger, Bolund, Magnussin, Lützén, & Andershed, 2008; Strickland et al., 2015). In the current study, patients’ extended family members played a significant role in helping them achieve their aims, particularly for those with younger children.
Families have been found to play an important role in supporting women with cancer in their efforts to balance the challenges of being a mother and being a patient (Coyne, Wollin, & Creedy, 2012). The current authors’ findings highlighted the importance of providing family-centered care to women undergoing stem cell transplantation. Nurses should provide opportunities for patients to talk about their feelings and concerns about the impact of cancer and its treatment on their children and their parenting (Elmberger et al., 2008). Efforts should also be taken to consider the dual demands of these patients when scheduling appointments and treatments (Fisher & O’Connor, 2012).
Late Effects and Survivorship
Many participants reported that their recovery took longer than they had expected, and some were still experiencing physical and psychological late effects at the time of the interviews. These included concerns about body image, fatigue, and sexuality, which, for some, had a negative impact on their physical relationships with their partners. Cancer and its treatment can result in sexual dysfunction, and many cancer survivors report not feeling prepared or adequately informed about these changes (Bober & Varela, 2012). Few of the women in the current study had discussed these issues with their healthcare team or sought advice, highlighting a significant gap in the current authors’ services.
Limitations
Retrospective interviews were used in the study, which prompted participants to recall earlier events. The womens’ descriptions of their experiences of diagnosis and treatment were influenced by the time that had passed since their treatment and subsequent events. Two of the participants recalled how they had difficulty remembering some of the symptoms. The sample size was small because the aim of the study was to explore the experiences of a limited number of patients in-depth; therefore, the findings cannot be generalized beyond this group of women with GTN. The themes identified were present across the interviews; however, additional insights may be provided by other participants. This study provided data that can be used to develop additional studies both in the United Kingdom with patients with GTN treated after 2013 and in collaboration with GTN services in other countries.
Implications for Nursing
The current study highlights the importance of communicating the process and challenges of stem cell transplantation in a way that ensures patients are better prepared for the difficulties they experience during and after treatment. Involving patients and their stories in this process could help ensure that interventions better match the reality of the patient experience.
The importance of considering the family context of women receiving stem cell transplantation was also identified. Participants had significant concerns about being separated from their children and the impact it would have on their well-being. Nurses need to be aware of the psychological consequences of this situation on patients and help them prepare for and cope with this aspect of treatment.
Health professionals need to be aware of the long-term consequences of cancer and its treatment. Byar, Eilers, and Nuss (2005) recommended that rehabilitation programs be implemented for survivors of high-dose chemotherapy. Survivorship and rehabilitation services are relatively new developments in cancer care, and a wealth of resources can be tapped into to support patients experiencing long-term effects (McCabe, Faithfull, Makin, & Wengstrom, 2013). The current findings have led to changes in local practice, and patients with GTN are now being referred to the late effects service as part of their routine treatment.
The current study identified areas for additional research. Participants were concerned for their children and their parenting role. Much of the research on this subject has been carried out among women with breast cancer, but the current findings suggest that the experiences of patients with parenting responsibilities receiving stem cell treatment, alongside potential nursing interventions that support them, warrant further investigation.
[[{"type":"media","view_mode":"media_original","fid":"32046","attributes":{"alt":"","class":"media-image","height":"229","typeof":"foaf:Image","width":"370"}}]]
Conclusion
The current study aimed to explore the experiences of women with GTN who underwent stem cell transplantation to understand their perspectives of treatment, priorities, and concerns. It revealed significant short- and long-term physical and psychological consequences affecting patients’ health and quality of life. The findings revealed particular service needs, including family-centered care, pretreatment preparation, rehabilitation, and late effects services. The importance of services developed with an understanding of the needs of women with this rare diagnosis was also identified. Additional research is needed with more women undergoing this treatment to better understand their experiences. The current study also provides insight that may be important to parents with other cancers undergoing intensive treatment.
The authors gratefully acknowledge Weston Park Hospital in Sheffield and Charing Cross Hospital in London for their support.
About the Author(s)
Singh is a lead nurse, Warnock is a practice development sister, and Ireson is a clinical nurse specialist, all at Sheffield Teaching Hospitals in South Yorkshire, England; Strickland is a clinical nurse specialist and Short is a speciality manager, both at the Imperial College NHS Foundation Trust in London, England; Seckl is a professor of medical oncology in the Department of Surgery and Cancer at Imperial College in London; and Hancock is a retired professor emeritus in the Medical School at the University of Sheffield in South Yorkshire. No financial relationships to disclose. Mention of specific products and opinions related to those products do not imply endorsement by the Oncology Nursing Society. Singh, Warnock, Strickland, Seckl, and Hancock contributed to the conceptualization and design and the manuscript preparation. Singh, Warnock, Ireson, Strickland, and Short completed the data collection. Singh and Strickland provided statistical support. Singh and Warnock provided the analysis. Singh can be reached at kamaljit.singh@sth.nhs.uk, with copy to editor at ONFEditor@ons.org. Submitted March 2016. Accepted for publication July 22, 2016.
References
Adelstein, K.E., Anderson, J.G., & Taylor, A.G. (2014). Importance of meaning-making for patients undergoing haemoatopoietic stem cell transplantation [Online exclusive]. Oncology Nursing Forum, 41, E172–E184. doi:10.1188/14.ONF.E172-E184
Alazzam, M., Tidy, J., Osborne, R., Coleman, R., Hancock, B.W., & Lawrie, T.A. (2012). Chemotherapy for resistant or recurrent gestational trophoblastic neoplasia. Cochrane Database of Systematic Reviews, CD008891. doi:10.1002/14651858.CD008891.pub2
Arès, I., Lebel, S., & Bielajew, C. (2014). The impact of motherhood on perceived stress, illness intrusiveness and fear of cancer recurrence in young breast cancer survivors over time. Psychology and Health, 29, 651–670. doi:10.1080/08870446.2014.881998
Bird, L., Arthur, A., Niblock, T., Stone, R., Watson, L., & Cox, K. (2010). Rehabilitation programme after stem cell transplantation: Randomized controlled trial. Journal of Advanced Nursing, 66, 607–615. doi:10.1111/j.1365-2648.2009.05232.x
Bober, S.L., & Varela, V.S. (2012). Sexuality in adult cancer survivors: Challenges and intervention. Journal of Clinical Oncology, 30, 3712–3719. doi:10.1200/JCO.2012.41.7915
Byar, K.L., Eilers, J.E., & Nuss, S.L. (2005). Quality of life 5 or more years post-autologous hematopoietic stem cell transplant. Cancer Nursing, 28, 148–157.
Choi, M.C., Lee, C., Smith, H.O., & Kim, S.J. (2015). Epidemiology. In B.W. Hancock, M.J. Seckl, & R.S. Berkowitz (Eds.), Gestational trophoblastic disease (4th ed.). Retrieved from http://bit.ly/2nER5sz
Coyne, E., Wollin, J., & Creedy, D.K. (2012). Exploration of the family’s role and strengths after a young woman is diagnosed with breast cancer: Views of women and their families. European Journal of Oncology Nursing, 16, 124–130. doi:10.1016/j.ejon.2011.04.013
El-Helw, L.M., Seckl, M.J., Haynes, R., Evans, L.S., Lorigan, P.C., Long, J., . . . Hancock, B.W. (2005). High-dose chemotherapy and peripheral blood stem cell support in refractory gestational trophoblastic neoplasia. British Journal of Cancer, 93, 620–621. doi:10.1038/sj.bjc.6602771
Elmberger, E., Bolund, C., Magnussin, A., Lützén, K., & Andershed, B. (2008). Being a mother with cancer: Achieving a sense of balance in the transition process. Cancer Nursing, 31, 58–66. doi:10.1097/01.NCC.0000305677.90963.67
Fisher, C., & O’Connor, M. (2012). “Motherhood” in the context of living with breast cancer. Cancer Nursing, 35, 157–163. doi:10.1097/NCC.0b013e31821cadde
Froeling, F.E., & Seckl, M.J. (2014). Gestational trophoblastic tumors: An update for 2014. Current Oncology Reports, 16, 408.
Lok, C.A., Singh, K., Fisher, R.A., Hancock, B.W., & Seckl, M.J. (2015, September). The results of treatment with high dose chemotherapy and peripheral blood stem cell support for ultra-high risk gestational trophoblastic disease. Paper presented at the International Society of the Study of Gestational Trophoblastic Diseases World Congress, Bali, Indonesia.
McCabe, M.S., Faithfull, S., Makin, W., & Wengstrom, Y. (2013). Survivorship programs and care planning. Cancer, 119, 2179–2186. doi:10.1002/cncr.28068
Mosher, C.E., Redd, W.H., Rini, C.M., Burkhalter, J.E., & DuHamel, K.N. (2009). Physical, psychological, and social sequelae following hematopoietic stem cell transplantation: A review of the literature. Psycho-Oncology, 18, 113–127. doi:10.1002/pon.1399
Ritchie, J., Lewis, J., Nicholls, C.M., & Ormston, R. (Eds.). (2013). Qualitative research practice: A guide for social science students and researchers. Thousand Oaks, CA: Sage.
Sarwar, N., Newlands, E.S., & Seckl, M.J. (2004). Gestational trophoblastic neoplasia: The management of relapsing patients and other recent advances. Current Oncology Reports, 6, 476–482. doi:10.1007/s11912-004-0079-1
Seckl, M.J., Sebire, N.J., & Berkowitz, R.S. (2010). Gestational trophoblastic disease. Lancet, 376, 717–729. doi:10.1016/S0140-6736(10)60280-2
Semple, C.J., & McCance, T. (2010). Parents’ experience of cancer who have young children: A literature review. Cancer Nursing, 33, 110–118. doi:10.1097/NCC.0b013e3181c024bb
Strickland, J.T., Wells, C.F., & Porr, C. (2015). Safeguarding the children: The cancer journey of young mothers. Oncology Nursing Forum, 42, 534–541. doi:10.1188/15.ONF.534-541
Sutherland, G., Dpsych, L.H., White, V., Jefford, M., & Hegarty, S. (2008). How does a cancer education program impact on people with cancer and their family and friends? Journal of Cancer Education, 23, 126–132. doi:10.1080/08858190802039177
Tidy, J. (2016, June). Comment made during the public meeting of the Choriocarinoma Service at the Clinical Outcome Collaborative Audit Workshop. Charing Cross Hospital, London.
Wenzel, L., Berkowitz, R.S., Newlands, E., Hancock, B., Goldstein, D.P., Seckl, M.J., . . . Higgins, J. (2002). Quality of life after gestational trophoblastic disease. Journal of Reproductive Medicine, 47, 387–394.
Wu, L.M., Austin, J., Hamilton, J.G., Valdimarsdottir, H., Isola, L., Rowley, S., . . . Rini, C. (2011). Self‐efficacy beliefs mediate the relationship between subjective cognitive functioning and physical and mental well‐being after hematopoietic stem cell transplant. Psycho-Oncology, 21, 1175–1184. doi:10.1002/pon.2012