Patients’ Experiences With Multiple Myeloma: A Meta-Aggregation of Qualitative Studies
Problem Identification: To systematically review qualitative evidence regarding patients’ experiences of living with multiple myeloma. The main objective was to gain structured understanding of this experience, which is a prerequisite for advancing nursing care and ensuring it is effective.
Literature Search: Qualitative research articles from January 2005 to March 2016 were located in CINAHL®, PubMed, and Scopus. Supplementary resources were found by scrutinizing reference lists and performing citation tracking. All included articles fulfilled predetermined criteria.
Data Evaluation: Three reviewers independently assessed the risk of methodologic bias by using the Joanna Briggs Institute (JBI) Qualitative Assessment and Review Instrument. The JBI methodology of meta-aggregation was used to synthesize findings.
Synthesis: Eleven studies fulfilled the eligibility criteria. From these, 84 findings were extracted. Each finding was assigned a level of credibility: unequivocal, credible, or unsupported. Findings were grouped into 11 subcategories and synthesized further into four main categories: (a) distress, (b) a different body, (c) coping, and (d) contributions of other people.
Conclusions: Patients with myeloma require a different form of follow-up compared to patients with many other cancers because of its chronic nature. Results demonstrate that widespread physical, emotional, and social challenges were experienced by patients throughout their illness trajectories, even in periods of remission. Nursing care should incorporate knowledge of patients’ experiences.
Implications for Practice: The results provide directions for nurses to improve supportive strategies in the care of patients with multiple myeloma. The categories provide a useful framework for developing clinical assessment tools.
Jump to a section
Patients diagnosed with multiple myeloma need to adjust to many changes throughout their illness trajectories. Although several qualitative studies have shown that the disease has a substantial impact on patients’ life situations and possibilities (Dahan & Auerbach, 2006; Kelly & Dowling, 2011; Maher & de Vries, 2011), no study has synthesized these research findings.
Multiple myeloma is a rare cancer in which plasma cells accumulate in the bone marrow and secrete an abnormal immunoglobin (paraprotein). Although only accounting for 1% of all cancer types, multiple myeloma is the second most common hematologic malignancy (Lobban & Perkins, 2013; National Comprehensive Cancer Network [NCCN], 2016; Stephens, 2009). Myeloma usually affects patients in late adulthood, which is reflected in the average age of 70 years at diagnosis (Genadieva-Stavric, Cavallo, & Palumbo, 2014). Advancements in treatment, with development of novel drugs used in combination with cytostatic therapy, autologous stem cell transplantation, and improved supportive care, has led to increased survival of patients with myeloma (Genadieva-Stavric et al., 2014; Röllig, Knop, & Bornhäuser, 2015). Despite these improvements, patients are still challenged with burdensome symptoms, both related to the disease itself and side effects of treatment, and, therefore, need to modify their daily life activities substantially (Jordan et al., 2014).
The clinical course of myeloma is characterized by fluctuations and unpredictability. After treatment, patients may experience periods of clinical remission, but they never know when the next exacerbation will occur. With time, patients may become entirely unresponsive to treatment (Lobban & Perkins, 2013). Typical symptoms that patients with multiple myeloma experience are fatigue, pain, neuropathy, and insomnia (Boland et al., 2013), along with complications such as bone lesions, hypercalcemia, anemia, kidney damage, and immunosuppression (Stephens, 2009).
Researchers have studied the health-related quality of life (HRQOL) of patients with myeloma at different time points. Even early in treatment, patients experience a considerable need for professional support—support that is not directed toward only treatment-related concerns. To illustrate, newly diagnosed patients who were eligible for intensive treatment, such as stem cell transplantation, described an array of concomitant physical and psychosocial symptoms such as emotional distress (e.g., anxiety, depression) and decreased functional performance (Coleman et al., 2011; Sherman, Simonton, Latif, Spohn, & Tricot, 2004). Similar results have also been found in those with longer disease duration (Jordan et al., 2014; Molassiotis, Wilson, Blair, Howe, & Cavat, 2011b). Current evidence shows that, at all phases of the disease, patients may experience a considerable symptom burden that negatively influences their HRQOL (Osborne et al., 2012). Other studies have shown that being in the first treatment-free interval (rather than other treatment phases) and longer periods of remission were associated with improvement in HRQOL (Acaster, Gaugris, Velikova, Yong, & Lloyd, 2013). In spite of a generally better situation during remission, patients are still required to deal with enduring problems (Boland et al., 2014).
Nurses have an important role in providing patients and their families with information and support, as well as in making holistic assessments of physical, practical, and emotional needs (Faiman, 2007). They play an important role in managing side effects and complications and helping patients and their loved ones with supportive care (Lobban & Perkins, 2013). This care aims to enhance HRQOL (Faiman, 2007; Lobban & Perkins, 2013; Stephens, 2009). To ensure that the care corresponds to patients’ expectations, nurses must gain insight into the multiple challenges that patients are confronted with. Therefore, research results should be structured in a pragmatic way that makes it possible to use them in clinical care.
The aim of this review was to synthesize results of existing qualitative studies on patients’ experience of living with multiple myeloma. The objective was to gain a comprehensive understanding of this experience so that nursing care can more accurately target patients’ needs. The research question was formulated according to the Sample, Phenomenon of Interest, Design, Evaluation, and Research type (SPIDER) tool (Cooke, Smith, & Booth, 2012): How do patients with multiple myeloma describe their experience of living with the disease, their daily challenges and helpful strategies, from diagnosis onwards, in existing qualitative studies?
Methods
The design of this review adhered to the Joanna Briggs Institute (JBI) methodology of meta-aggregation to allow a systematic synthesis of qualitative evidence of patients’ experiences with multiple myeloma. Although the method of meta-aggregation mirrors the processes of a quantitative review, it retains the characteristics of qualitative research traditions (Hannes & Lockwood, 2011; JBI, 2014). Also, rather than reinterpreting findings of primary qualitative studies, this methodology discovers the practicality and usability of research findings across studies (JBI, 2014; Korhonen, Hakulinen-Viitanen, Jylhä, & Holopainen, 2013). To ensure clear reporting of the method, review findings, and implications, the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) protocol was followed (Liberati et al., 2009).
Search Strategy
The search strategy was structured according to SPIDER to enable more precision in the search strategy and location of relevant studies to answer the research question (Cooke et al., 2012).
A preliminary search was conducted using the Cochrane, JBI, PubMed, and Google Scholar® databases to identify the presence of existing systematic reviews. No existing syntheses of qualitative studies were found. Therefore, a systematic search was conducted in PubMed, CINAHL®, and Scopus. Additional studies were located by scrutinizing the reference lists of included studies and performing citation tracking in Google Scholar. A representation of the search process can be found in Figure 1. 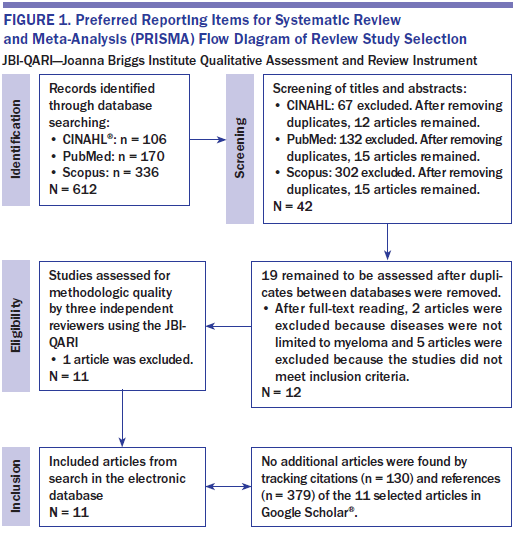
Eligibility Criteria
Studies were deemed eligible if they were published peer-reviewed qualitative studies on patients’ experiences of living with multiple myeloma. Study populations had to be adult (aged 18 years or older) and diagnosed with multiple myeloma at any stage of the disease. Only English-language studies were considered, with a publication date from January 2005 to March 2016. Older studies were excluded because of advancements in treatments, which have led to increased survival (Genadieva-Stavric et al., 2014). Studies with unsupported results, such as unclear themes and/or lack of participants’ quotations, were excluded.
Study Selection
All abstracts were screened for suitability by the first author (BH). Full-text articles were retrieved for the chosen abstracts. Two authors (BH/KB) independently assessed the articles in their entirety, matching them against the inclusion criteria and evaluating the risk of methodologic bias. A third reviewer (MK) validated their findings. Any disagreement was resolved by consensus. Additional resources were found by scrutinizing the reference lists of included studies and conducting citation tracking. Potential new studies identified through this process were subjected to all of the previously mentioned steps. All full-text articles that initially were rejected went through a second evaluation by all authors to ascertain whether that rejection was justified.
Quality Appraisal
Methodologic quality was assessed using the 10-item standardized critical appraisal instruments from the JBI Qualitative Assessment and Review Instrument (JBI-QARI) (JBI, 2014). This appraisal was used by the researchers to guide the interpretation and presentation of the results.
Data Extraction and Synthesis
Data extraction and synthesis were accomplished in agreement with the four phases of meta-aggregation: (a) gathering findings, themes, metaphors, and categories from all studies; (b) aggregating findings based on similarity in meaning and by placing them into relevant subcategories; (c) merging subcategories into main categories; and (d) presenting results in a way that provides pragmatic lines of action (Hannes & Lockwood, 2011; JBI, 2014).
Results
Selected Studies
The electronic database search found 612 potential articles. A total of 19 articles remained after screening the titles and abstracts and adjusting for duplicates within and between databases. Ultimately, 11 studies were included (see Table 1). 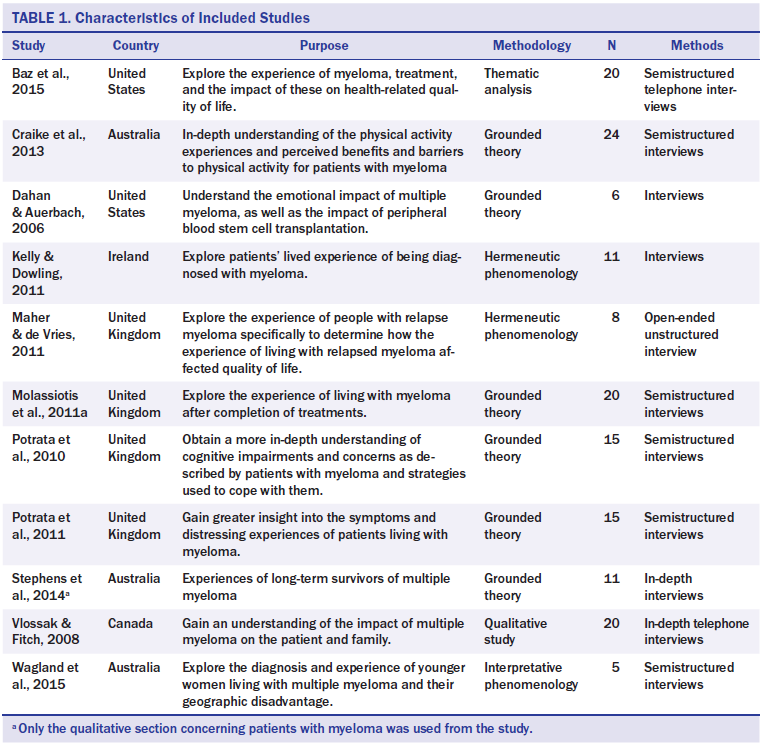
The studies included a total of 140 patients. The most common qualitative methodology of the reviewed studies was grounded theory. Two studies used the same participants. However, their results revealed different facets of the myeloma experience. The study by Potrata, Cavet, Blair, Howe, and Molassiotis (2010) focused primarily on cognitive impairments, whereas Potrata, Cavet, Blair, Howe, and Molassiotis (2011) concentrated on other distressing experiences.
Assessment of Methodologic Quality
From the 11 included studies, 84 findings were extracted. All of these findings were appraised as being unequivocal, apart from one that was found to be credible (see Table 2).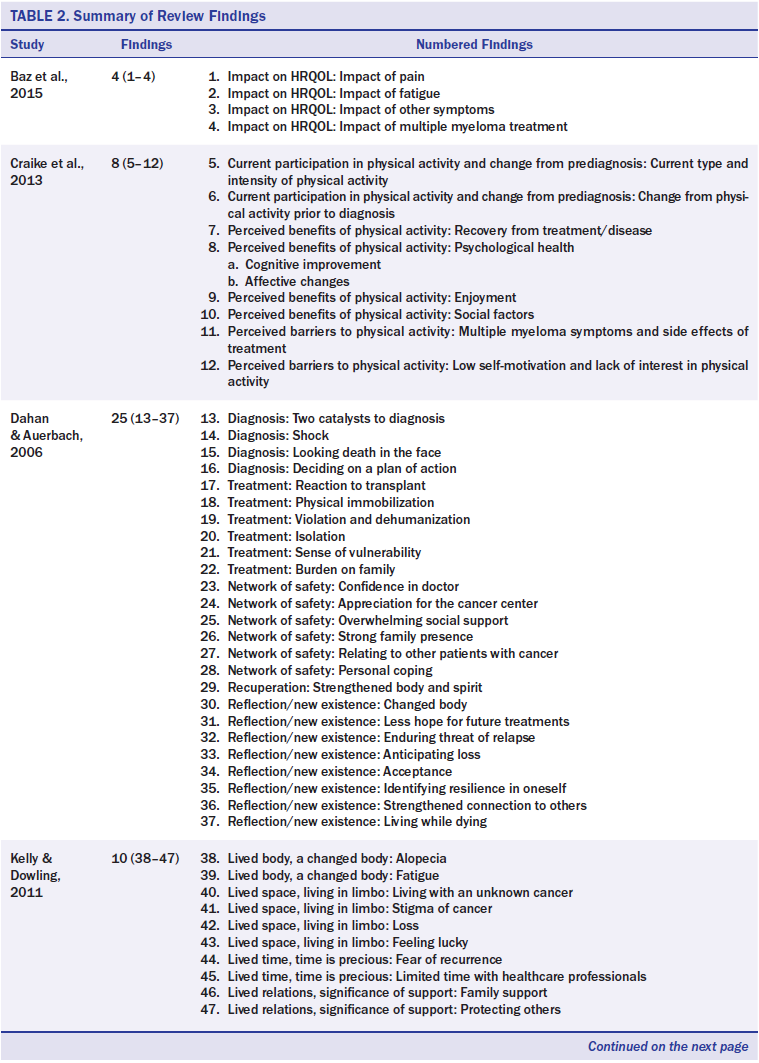
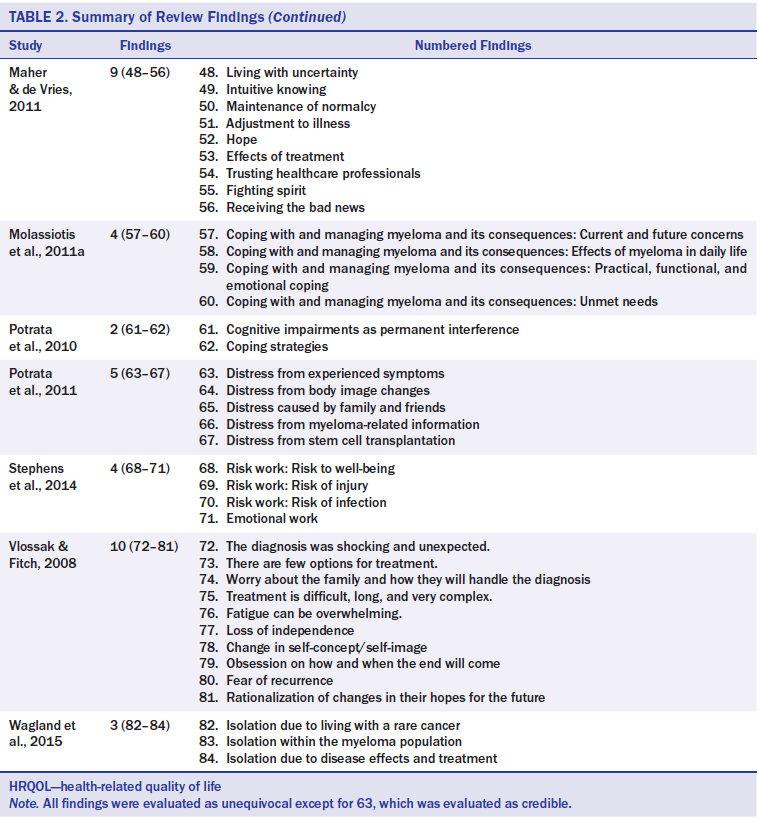
The 84 findings were grouped into 11 subcategories from which four main categories emerged, reflecting the experience of living with myeloma. The presentation of results is similar to a previous review using similar methodology (Burckhardt, Belzner, Berg, & Fleischer, 2014). In the following sections, major results within each of the four synthesized categories are described. Illustrative quotations are presented from the original studies within the four main categories respectively, along with their relevant references (see Appendices A–D).
Synthesis 1: Distress
This synthesis is based on 28 findings grouped into four subcategories (see Figure 2).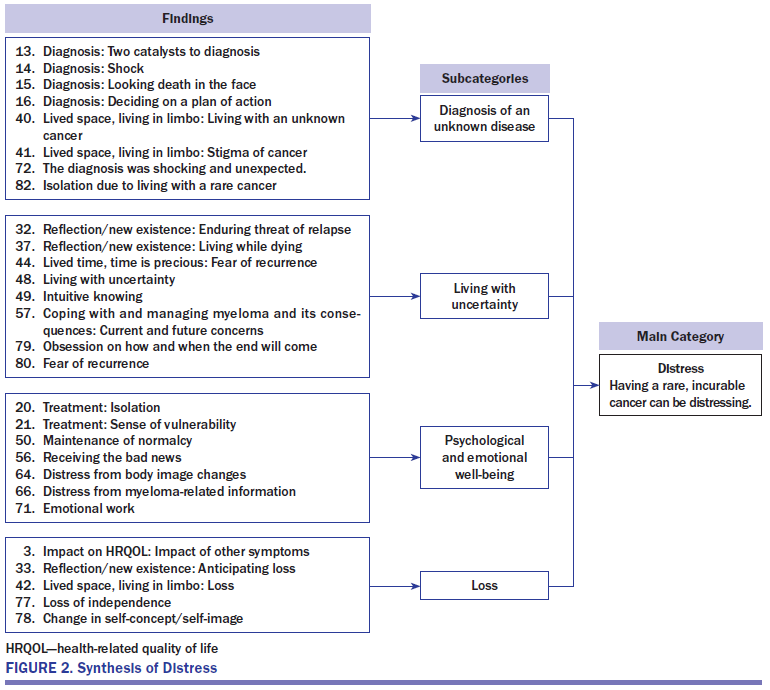
Diagnosis of an unknown disease: Receiving the diagnosis of myeloma was a huge blow, where patients experienced a sudden confrontation with their own mortality. Life had changed forever. Most had never heard of the disease prior to diagnosis and were uncertain of what challenges they would be confronted with. The fact that other people also lacked knowledge of the disease prevented the patients from receiving questions and feedback from their friends and family. This accentuated the strangeness and feeling of isolation in initiating a changed life with myeloma. One of the first actions that patients carried out after receiving their diagnosis was to gather useful information about the disease and its possibilities for treatment. It was important for them to become well acquainted with the disease.
Living with uncertainty: Living with an incurable cancer and a relentless threat of relapse was a difficult experience that was always at the back of the patients’ minds. The patients tried not to let this prospect control their entire existence. Attending routine hospital appointments increased their awareness of the disease and tended to aggravate fear and uncertainty concerning disease progression and the availability of treatment.
Psychological and emotional well-being: Myeloma had a substantial impact on patients’ well-being. Patients described isolation that was heavily influenced by feelings of being different. This isolation became more pronounced when simultaneous withdrawal from social activities occurred. Patients felt that they had to be brave and be able to control their emotions, which was not always possible. Having to repeat bad news to family and friends was difficult and stressful. It was of great importance to patients to maintain their normal lives and not let the cancer become the dominant factor. This, however, proved to be a difficult, ongoing task. Hair loss, changes in weight, brittle bones, and other symptoms caused by the disease or the treatment were often a source of distress to the patients and made them feel vulnerable. The visible indicators of sickness negatively impacted patients’ self-image.
Loss: Feelings of loss were related to changes in temporal expectations. These involved perceptions of missing out on or anticipating absence from significant life events with family, and also loss of identity and value. Patients experienced loss of independence and described not being able to do what they used to do, such as working or performing daily household chores. This loss of independence led to changes in self-esteem and made some patients feel useless.
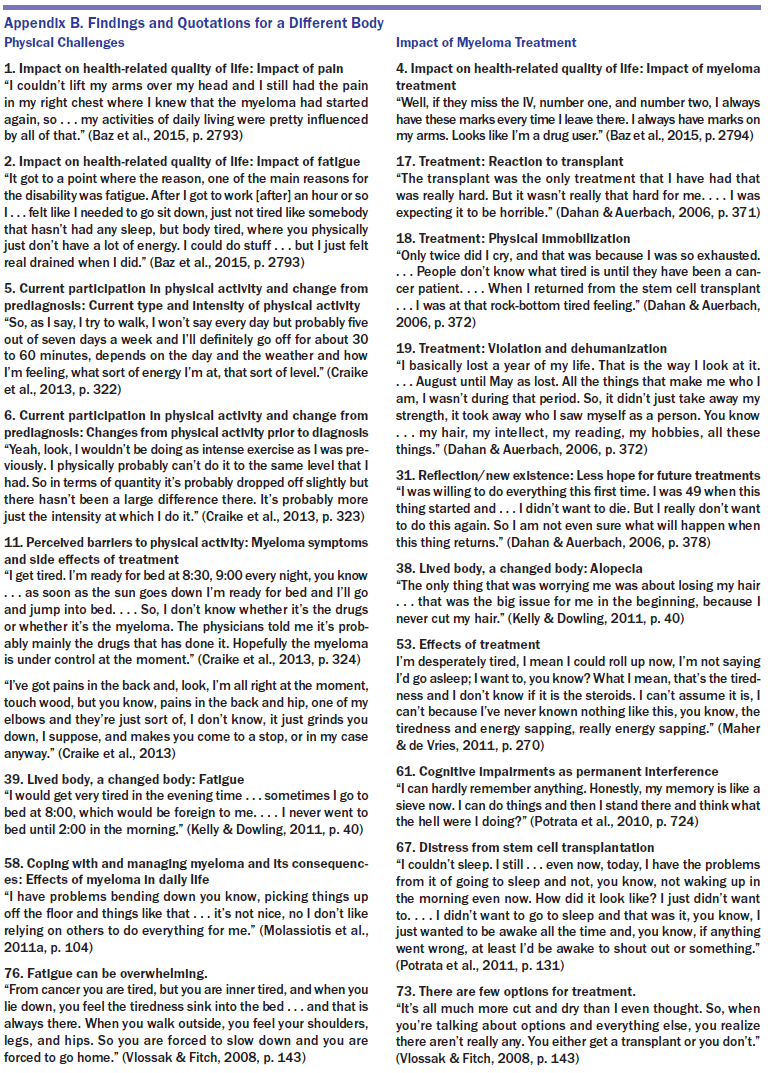
Synthesis 2: A Different Body
This synthesis is based on 22 findings grouped into two subcategories (see Figure 3). 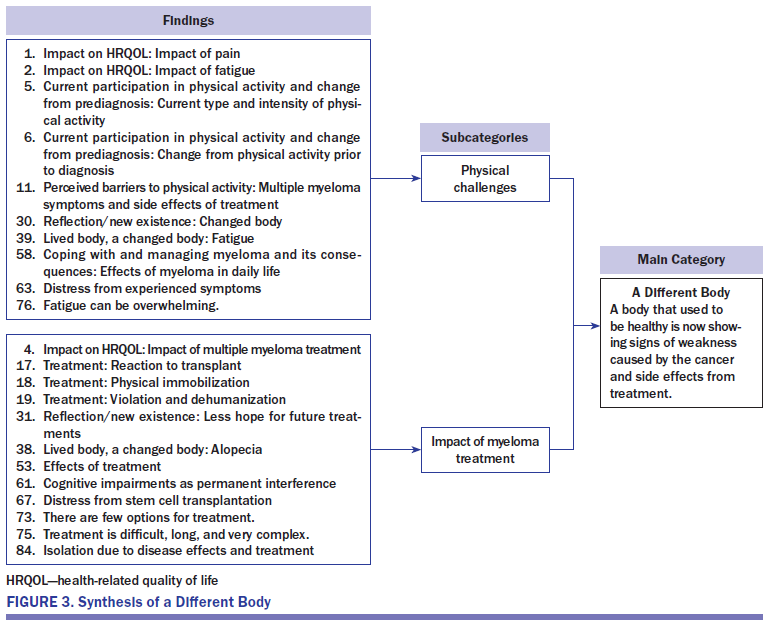
Physical challenges: Fatigue affected patients’ ability to participate in life and was described as one of the main obstacles that caused disability. Although patients were usually physically capable of doing daily chores, their lack of endurance required them to prioritize the situations in which to spend their sparse energy. Some could predict which activities would cause exhaustion, but, for others, unpredictable circumstances, lack of general well-being, or even changes in weather conditions adversely influenced their energy levels. Profound fatigue was a common consequence of treatment.
Pain largely affected patients’ lives in the same manner as fatigue. In particular, back pain commonly occurred. However, new pain was also associated with a warning sign of relapse and, therefore, caused additional concern. Collectively, fatigue and pain prevented patients from taking part in desired activities and hindered them physically and socially. Other physical symptoms mentioned were fragile bones, difficulties with movement, infections, neuropathy, hearing loss, bowel problems, and insomnia.
Impact of myeloma treatment: Patients who had undergone different types of treatment (i.e., standard chemotherapy, novel drugs, radiation or high-dose therapy with stem cell transplantation) experienced a wide variety of adverse symptoms. These ranged from marks from IV needles and loss of hair to others such as nausea, neuropathy, and fatigue. Being drained of energy also impaired patients’ cognitive function and memory. Although many described their treatment negatively, they felt forced to go through with it because it was their only option. People could not always predict how treatment would affect them; the different treatments and different time points of treatments could vary, from being without complications altogether to having all-encompassing effects on well-being.
Patients were prepared to accept profound adverse side effects if the treatment was effective, but with many relapses, such enthusiasm became difficult to maintain. The perception of freedom became constrained when the treatment affected physical strength, appearance, leisure activities, mental function, and other personal factors. In addition, a weak immune system required patients to discourage friends and family from visiting them to protect themselves from catching contagious common diseases or viruses.
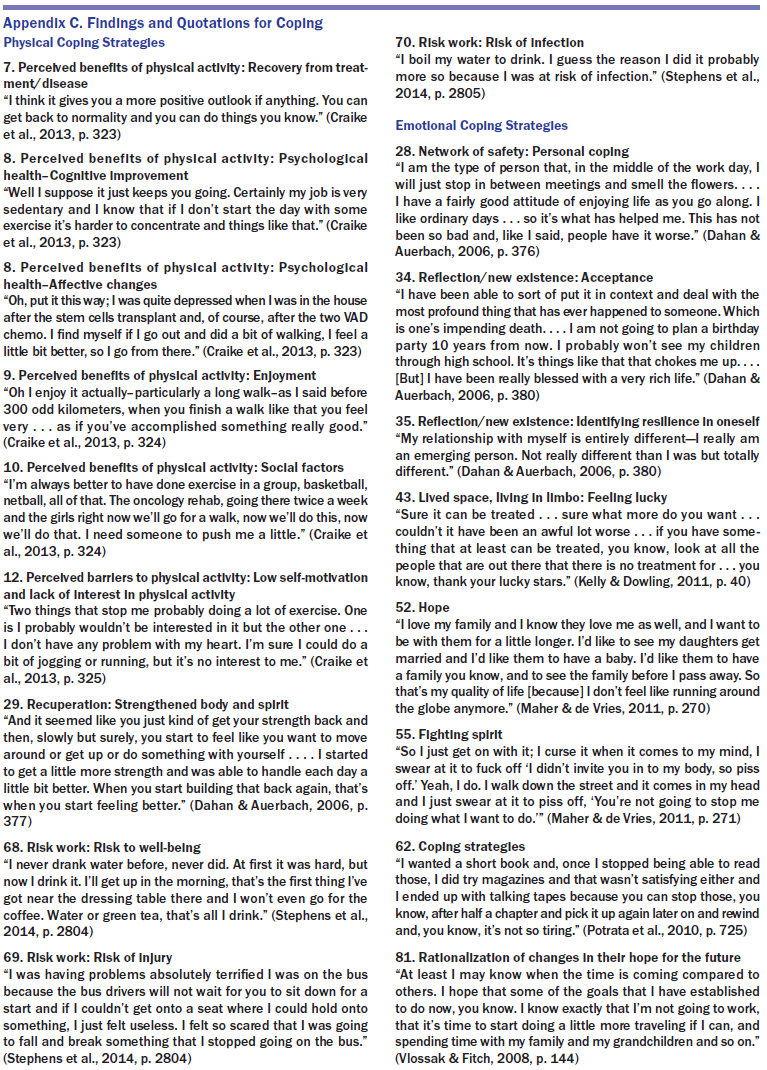
Synthesis 3: Coping
This synthesis is based on 18 findings grouped into two subcategories (see Figure 4). 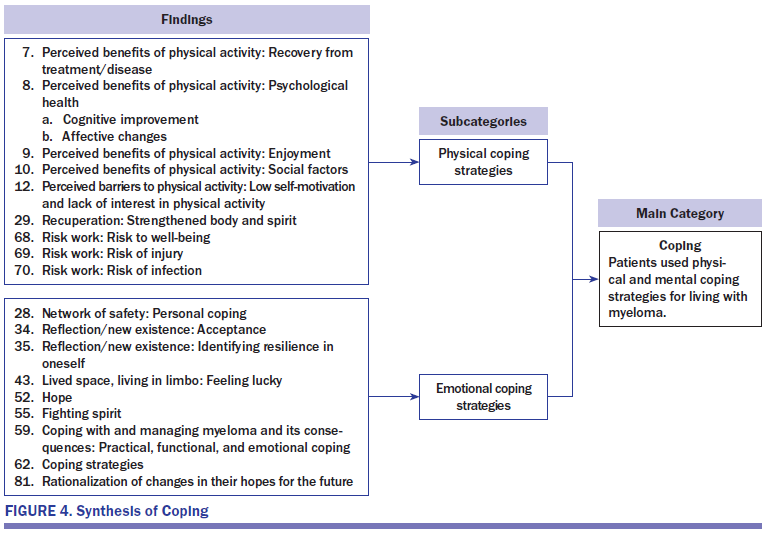
Physical coping strategies: Patients looked for ways to retain or increase their physical health. They used various approaches, including eating healthier food, drinking more water, and exercising. To prevent infection, some patients boiled their drinking water and avoided situations that would upset the precarious balance of physical well-being. Although exercising was sometimes difficult, it left the patients with a victorious feeling when they succeeded in pushing their physical boundaries and regaining control of their bodies. When recovering from side effects of treatment, physical activity had several benefits, such as improving memory and concentration. In addition, physical activity made them feel better and decreased isolation. Staying on schedule for exercise also gave them a feeling of being in control. However, some people lacked motivation and were dependent on encouragement from others, such as healthcare professionals, to find motivation for activities that they could engage in. Other physical coping strategies focused on minimizing risk of physical harm related to injury caused by peripheral neuropathy and fragile bones. For example, some stopped using public transportation because of the risk of falling and fracturing brittle bones.
Emotional coping strategies: Emotional coping strategies were used to stay optimistic and preserve hope in spite of the uncertainty of living with myeloma. Some found this resilience within themselves and focused on enjoying their lives. Some reported feeling fortunate to have a diagnosis and, knowing that time was precious, this helped patients to prioritize and to make the most of their lives. It was important for patients to establish hopes for future experiences, such as having grandchildren. Comparing their own situations to those of others who were less privileged also was a way of realizing that things could be worse. Although myeloma was not curable, treatment was available.
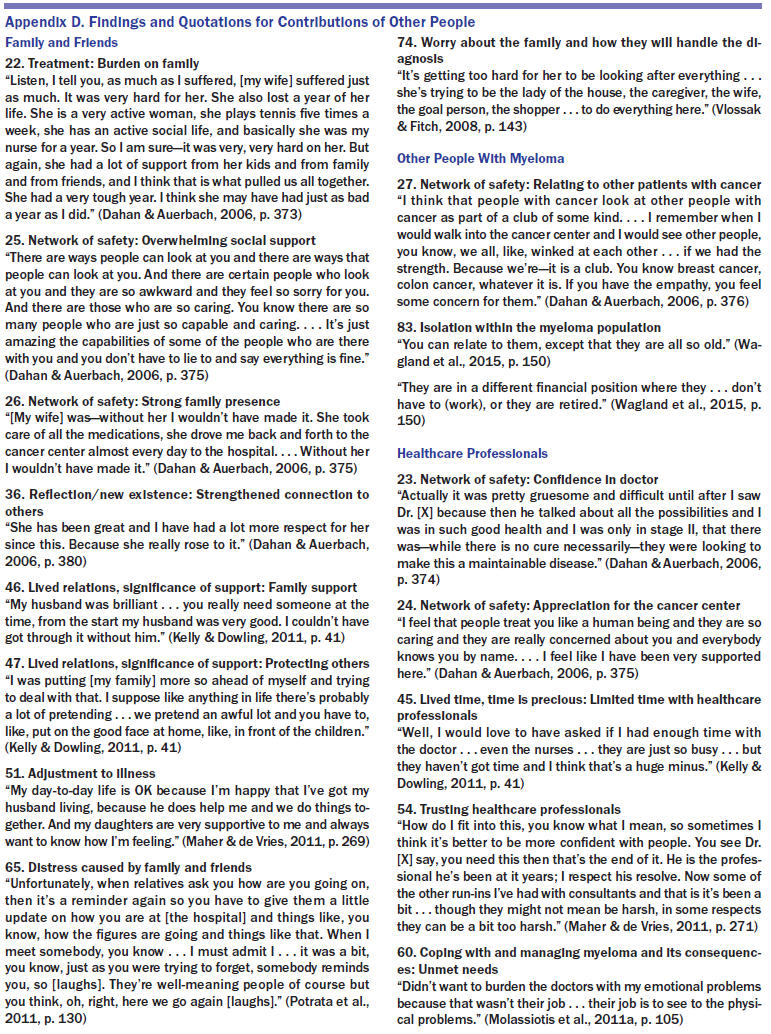
Synthesis 4. Contributions of Other People
This synthesis is based on 16 findings grouped into three subcategories (see Figure 5). 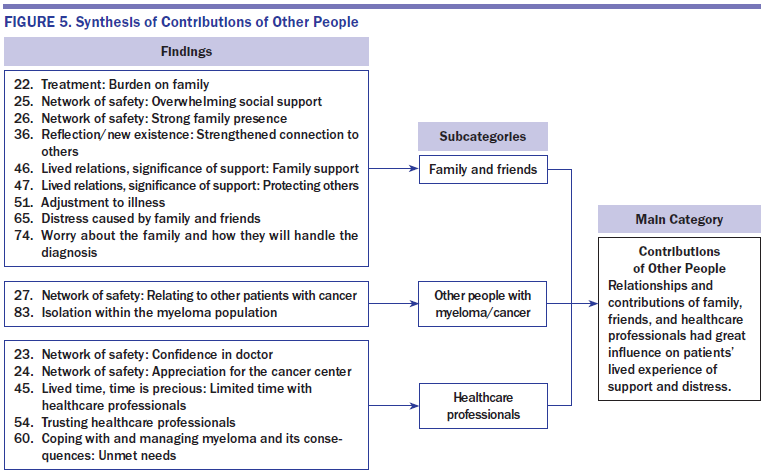
Family and friends: The spouses usually provided the most support, both psychologically and with practical chores such as cooking, driving to and from treatment sessions, and so forth. However, other close relationships were also important. Having access to a group of people where it was possible to express feelings freely could provide relief. On the other hand, patients sometimes felt required to shield other people, such as their children, from seeing their suffering.
Although family and friends provided an appreciated network of safety and support, they also caused concern (e.g., repeatedly inquiring about the patient’s health and well-being). This increased awareness of their disease at time points when they did not want to contemplate it. Patients also worried about how the increased burden on their families and their future death would affect their loved ones.
Other people with myeloma/cancer: Some patients were interested in talking to others with myeloma about their experience with the disease, but not all had the chance to do so. Because myeloma is usually diagnosed in older adult populations, younger patients did not feel that they had much in common with the majority of other patients, which could lead to feelings of isolation.
Healthcare professionals: Patients most frequently described a trusting relationship between themselves and the healthcare professionals involved in their care. However, limited time was available for the patients to talk to healthcare professionals. These time constraints prevented patients from raising questions and discussing their concerns, although they felt the need to do so. In particular, enduring problems that could not be managed well, such as fatigue, pain and mobility, were issues that patients refrained from discussing with professionals because they did not have positive experiences of receiving information that they could transfer into use in their daily life situations. Other sensitive issues impacting the patients’ lives were far too rarely discussed with healthcare professionals on the patient’s own initiative, such as changes in intimacy and emotional issues. Patients had most contact with healthcare professionals during relapses, and the focus then was on the disease, namely treatment options, monitoring worsening symptoms, and side effects of medication. At times of remission, patients often felt forgotten by the healthcare system.
Discussion
The results from this qualitative review show discrete components in patients’ experiences of a life with multiple myeloma. The wide-ranging impact of myeloma on patients’ physical, emotional, and social lives that was described, and the illustrations of actions that patients have taken to relieve their symptoms, easily translate into applications in clinical nursing practice. Patients with myeloma need access to ongoing professional support, even in times of remission. The four main categories—distress, a different body, coping, and contributions of other people—might serve as a launchpad for developing new ways of assessing fluctuations and problems of importance associated with myeloma. In the following sections, some major issues within each main category will be discussed, particularly to highlight the clinical implications of the findings in relation to existing knowledge.
Distress
Distress had the most well-described findings, indicating the importance of healthcare professionals’ awareness of the emotional burden that follows a diagnosis of myeloma. NCCN (2016) proposed the following definition of distress:
Because of the profound impact of distress, it often is viewed as the sixth vital sign (Estes & Karten, 2014). The participants across the 11 studies exhibited a broad spectrum of psychological and emotional symptoms. Most predominant were feelings of loss, sadness, anxiety, uncertainty, and isolation. In many instances, these feelings restricted the participants’ lives substantially, and, as such, call for professional attention. Many patients go without the psychosocial care that they require because of under-recognition of their distress. However, patients may also under-report such symptoms because of a fear that others may equate symptoms of distress to mental health problems (NCCN, 2016). A review article by Zabora, BrintzenhofeSzoc, Curbow, Hooker, and Piantadosi (2001) estimated that as many as 43% of patients with cancer are distressed and emphasized that this distress should be evaluated routinely. Nurses have been identified as the most relevant group of healthcare professionals to assess distress in patients with cancer (Abrahamson, 2010), and clinical guidelines recommend routine screening (NCCN, 2016). The distress described in the participants of the included studies further underscores the need to prioritize the identification of distress to enable the initiation of alleviating actions.
A Different Body
This category provided descriptions of physical symptoms and side effects that patients were challenged with. In congruence with other studies, fatigue and pain were commonly experienced (Coleman et al., 2011; Jordan et al., 2014; Sherman et al., 2004). Through this review, the importance of recognizing the presence of these symptoms and asking patients about them was reinforced, particularly because the symptoms were not always distinguishable despite having a substantial adverse effect on patients’ daily lives. Patients generally lacked advice on how to cope with symptoms that were not directly related to worsening in their medical condition and often refrained from seeking advice on their own initiative. This shows that nurses should be proactive in assessing for diverse problems impairing patients’ HRQOL. Current HRQOL scales for patients with myeloma address many important symptoms (e.g., bone aches and pain in other areas, side effects of treatment, worries) (Boland et al., 2013); however, they do not assess how these symptoms restrict the lived space—activities, connection to other people, possibilities, and well-being of patients. However, the difficulties of providing meaningful solutions to problems without having access to knowledge of how symptoms impede patients’ experiences is well recognized (Gapstur, 2007). Therefore, healthcare professionals should bear in mind that assessment should go beyond descriptions of symptom strength and consistency to include evaluation of the patients’ experience of them (McMillan, Tofthagen, Choe, & Rheingans, 2015). Nursing guidelines predominantly target issues that are related to the management of side effects of treatment and problems that appear with deterioration (Bertolotti et al., 2008; Bilotti et al., 2011). Therefore, development of more all-encompassing assessment and management strategies should be given priority (Lobban & Perkins, 2013).
Coping
Coping reflects strategies that patients used to maintain some kind of equilibrium in a life with myeloma. The participants said that only a few—if any—previous life experiences had led to more fear than receiving their diagnosis. The diagnosis brought them into proximity to a threat against their own existence, difficult decisions with regard to treatments, and more. When people are diagnosed with myeloma or other forms of cancer, this creates a sudden need to redefine previous priorities and find ways to cope with uncertainty (Hoffman, Lent, & Raque-Bogdan, 2013). Research has shown that such goal reengagement, when it is most successful, can result in psychological satisfaction and positive life changes (Schroevers, Kraaij, & Garnefski, 2011). A concept analysis of learning to live with a chronic disease revealed this as a complex, dynamic, cyclical, and multidimensional adjustment process where the ultimate target was to achieve positive living and to maintain one’s own self-identity (Ambrosio et al., 2015). The current authors found that the participants used two basic kinds of coping strategies, physical and mental. The physical strategies focused on strengthening and safeguarding their vulnerable body, whereas the mental strategies related to finding and keeping up their fighting spirit, discovering inner peace, appreciating the good things in life, and developing hope and faith. This finding has many clinical implications. In their support of patients with myeloma, nurses may function as a catalyst for this adaptive process by helping patients to make explicit the things that they appreciate in life and by helping them to establish new manageable benchmarks.
Contribution of Other People
In this category, patients described how the relationships and contributions of family, friends, and healthcare professionals greatly influenced their experience of illness. Generally, this support facilitated good experiences. Patients’ personal networks helped to relieve them from performing daily activities and habitual chores and provided psychological and emotional support at difficult times. However, patients expressed profound worries, in particular those with more severe disease, that their illness was too much of a burden for their relatives. In the care of patients with myeloma, keeping in mind that patients’ challenges affect the caregivers, and vice versa, is important. Because of this interdependent relationship, healthcare professionals should consider the patients and informal caregivers as one unit (McLeod, Tapp, Moules, & Campbell, 2010; Northouse, 2012).
Most patients with myeloma repeatedly mentioned how busy they felt the healthcare professionals were, which hindered patients from communicating how they were feeling. This indicates that nurses should strive to not miss important clues related to what may improve the care of patients with myeloma and their families.
Limitations
The authors found a lack of qualitative studies with a longitudinal design to enable better descriptions of fluctuations and experiences in various phases of the disease. For instance, only one study explicitly described experiences of long-term survivors with myeloma (Stephens, McKenzie, & Jordens, 2014). Because of this underrepresentation, it remains uncertain whether patients in the end phase of the disease may have other needs and experiences. This issue calls for further research.
Although the authors adhered to a methodically strict procedure, several limitations must be mentioned. The authors only included studies reported in English and, therefore, more material may be available in other languages. Also, the authors did not perform manual searches of selected cancer journals. In looking further into patients’ needs, it may have been fruitful to access other kinds of literature, for instance, patient helplines and home pages of patients’ associations, and to conduct content analysis of this material. However, such analysis would have demanded more resources.
The transferability of the results may be influenced by the selection of patients from the original studies. Of note, the average age of the participants in the review studies was lower than the average age of patients with myeloma in general, and all patients had resources and energy enough to participate in the studies.
Implications for Nursing
The findings provide an important resource for clinical practice and can be used to improve care for people with myeloma. Although myeloma is chronic in nature, it fluctuates between remissions and relapses. Unsurprisingly, the focus of care has mostly been on patients with myeloma in its more aggressive phase. The evidence provided in this review demonstrates a need for nurses to put further emphasis on implementation of alleviating strategies in the remission stage of myeloma.
The four main categories of distress, a different body, coping, and contributions of other people, cover important items that could be incorporated in an assessment tool suitable for both the active and passive state of myeloma to allow patients to make explicit their own evaluation of their experience. Prevailing HRQOL instruments have not been developed based on qualitative findings and may, therefore, be criticized for paying too little attention to what really matters to patients (Osborne et al., 2012). A scale taking into consideration the qualitative findings could potentially measure the impact of fluctuations, establish particularly vulnerable periods, and assess the effectiveness of alleviating interventions. The scale would be a vital supplement to the application of more conventional screening methods (e.g., the Distress Thermometer [NCCN, 2016]).
Nurses should reach out to patients because patients do not seem to approach healthcare professionals about perceived minor issues impairing their well-being. Nurses could more specifically help patients with focusing on what they can do. Better access to specialized nursing care could, for instance, occur though a telephone service (Reid & Porter, 2011), interactive web-based interventions (Kuijpers, Groen, Aaronson, & van Harten, 2013), or homecare support service. These are pragmatic ways to optimize nursing support and to provide this support in a manner that transfers into use in patients’ daily life situations. 
Conclusion
The results of this review show the impact that multiple myeloma has on various aspects of patients’ lives, including physically, psychologically, and socially. Nursing care for patients with myeloma should match their experiences and existential needs. The contents within the main categories have a practical value in that they provide nurses with understanding of the challenges that these patients face. This knowledge has direct implications for clinical care provision. In addition, the structure derived from this meta-aggregation provides a useful framework for developing a clinical assessment tool that could help to identify patients in need of alleviating support throughout the continuum of care. 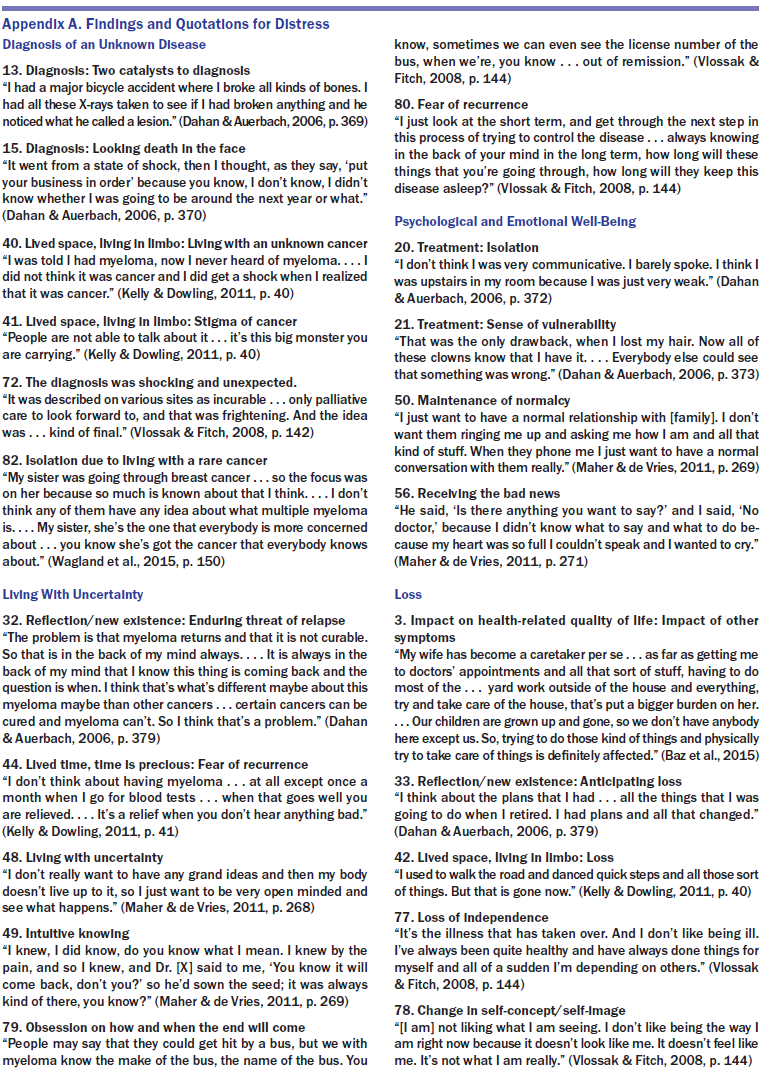
About the Author(s)
Hauksdóttir is an RN in the outpatient hematology-oncology department at the National University Hospital of Iceland; Klinke is a postdoctoral researcher in the Faculty of Nursing of the School of Health Sciences at the University of Iceland; Gunnarsdóttir is the chief nursing executive at the National University Hospital of Iceland and an associate professor in the Faculty of Nursing of the School of Health Sciences at the University of Iceland; and Björnsdóttir is a professor and senior researcher in the Faculty of Nursing of the School of Health Sciences at the University of Iceland, all in Reykjavík. No financial relationships to disclose. All of the authors contributed to the study conception and design. Hauksdóttir, Klinke, and Björnsdóttir performed the data analysis. Hauksdóttir carried out the literature searches and drafted the manuscript. Hauksdóttir can be reached at brynjaha@lsh.is, with copy to ONFEditor@ons.org. Submitted April 2016. Accepted for publication June 6, 2016.


