Symptom Assessment in Hospitalized Older Palliative Patients With Cancer: Agreement Among Patients, Nurses, and Proxies
Purpose/Objectives: To evaluate the level of agreement of symptom assessment among older adult palliative patients with cancer, nurses, and patients’ proxies.
Design: A cross-sectional study.
Setting: Two general hospitals in Flanders, Belgium.
Sample: 120 palliative patients with cancer, aged 65 years and older.
Methods: A validated 36-item instrument developed to assess physical, psychological, functional, social, and existential symptoms in older palliative patients with cancer was independently completed by patients, the nurses, and proxies.
Main Research Variables: Frequency and intensity of 36 symptoms.
Findings: The study indicates that nurses and proxies tend to underestimate physical and social symptoms and overestimate psychological, functional, and existential symptoms. Agreement scores between patients and nurses and patients and proxies were only significantly different in 39% and 20% of the cases, respectively. Higher intraclass correlation coefficients were measured between patients and proxies compared to patients and nurses. Agreement was associated with demographic and clinical factors, such as gender and prognosis.
Conclusions: This study indicates discrepancies among patient, nurse, and proxy in the assessment of symptoms.
Implications for Nursing: Patients should be encouraged to report their true experiences. Nurses and proxies should be taught to recognize and assess symptoms and to communicate about them with patients.
Jump to a section
Palliative care is defined as “an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual” (World Health Organization [WHO], 2002, pp. 15–16). Cancer remains one of the leading causes of death (Ferlay et al., 2010); therefore, patients with cancer represent an important proportion of the patients in the palliative care setting.
Palliative patients with cancer suffer from multiple symptoms and, at times, with high prevalence (Teunissen et al., 2007; Van Lancker et al., 2014). Subsequently, symptom management is seen as the most important aspect of palliative care (WHO, 2002). This requires adequate symptom assessment, which allows identification of symptoms in multiple domains, such as physical, psychological, social, functional, and existential (WHO, 2002). Like palliative care, care of older adults requires a multifaceted approach. Older adults often are confronted with comorbidities, polypharmacy, functional decline, cognitive problems, and loss of homeostatic reserve, which can result in symptoms in multiple domains (Depp & Jeste, 2006; Marengoni et al., 2011). Adequate symptom assessment is essential to be able to implement appropriate interventions to control symptoms.
Patient self-reported symptoms are seen as the gold standard in symptom assessment (Pautex, Berger, Chatelain, Herrmann, & Zulian, 2003). However, patients are not always able to report their symptoms because of a variety of reasons that are particularly relevant for older adult patients in palliative care (Kaye, Baluch, & Scott, 2010). Patients are, for instance, not able to report their symptoms if they experience cognitive problems, confusion, and weakness (Kaye et al., 2010; Nekolaichuk et al., 1999). For those patients, symptoms can only be assessed indirectly or estimated by a formal (nurse and physician) or informal (proxy) caregiver. The validity and reliability of those assessments are unclear. As a result, underreporting may result in undertreatment and overreporting may lead to unnecessary interventions, such as high doses of medication (Kaye et al., 2010; Winn & Dentino, 2005). This may reduce the quality of life of the patient and lead to discomfort.
Studies on the agreement of symptom assessment among the patient, the healthcare provider, and the proxy have been performed in different settings and populations (Higginson & Gao, 2008; Laugsand et al., 2010; Pautex et al., 2003; Yip, Wilber, Myrtle, & Grazman, 2001). To the authors’ knowledge, only one study focused on a population of older adult palliative care patients (Pautex et al., 2003). Overall, healthcare professionals and proxies have a tendency to under- and overreport symptoms, respectively. Lower agreement has been observed for more subjective symptoms, such as depression, and less prevalent symptoms, such as poor sleep (Laugsand et al., 2010; Pautex et al., 2003). In a population of older palliative patients, Pautex et al. (2003) used the Edmonton Symptom Assessment Scale (ESAS) and confirmed that healthcare providers tend to underestimate physical and objective symptoms and overestimate physiological and subjective symptoms. However, Pautex et al. (2003) assessed only a limited number of symptoms with a small sample size (N = 42).Therefore, the aim of the current study was to evaluate the level of agreement of symptom assessment (physical, psychological, functional, social, and existential) among older palliative patients, nurses, and proxies.
Methods
A cross-sectional study was performed from November 2012 to May 2013. The study was conducted in two general hospitals in Flanders, Belgium: General Hospital Groeninge, Kortrijk, and General Hospital OLV Lourdes, Waregem. Patients were recruited from eight internal medicine units and one geriatric ward.
A convenience sample of older palliative patients with cancer participated in the study. Patients were eligible for the study if they met following criteria: (a) aged 65 years or older; (b) a palliative patient as defined by Desmedt et al. (2011), “A patient suffering from an incurable, progressive, life-threatening disease, with no possibility of obtaining remission, stabilization or improvement of this illness” (p. 3); (c) having a current diagnosis of a malignant disease; (d) being able to interact with the interviewer; (e) being able to provide written, informed consent; and (f) being hospitalized for at least one week so that the nurses could make an adequate estimation of the occurrence of symptoms. The patient indicated a proxy who was able to provide an accurate estimation of the occurrence of symptoms. Patients were excluded if they had not received any visits in the past week and if they were in a terminal phase of illness (defined as the last phase of life and characterized by general organ failure).
Instruments
Symptoms were assessed using a validated 36-item instrument specifically designed for older palliative patients with cancer (Van Lancker et al., 2012). The instrument was developed based on an extensive literature review. Face and content validity were evaluated using a double Delphi procedure with 11 clinical and/or research experts in oncology, palliative care, geriatric care, and nursing. The item content validity index (I-CVI) ranged from 89.9%–100%. Lynn (1986) recommended an I-CVI of 80% or greater. The scale content validity index (S-CVI) was 93%. Polit and Beck (2011) recommended a S-CVI of 90% or greater. The instrument was pilot tested for clarity and ambiguity in a sample of 10 hospitalized older adult patients. Changes were made following the Delphi and pilot study. The instrument assesses symptoms on five domains: physical, psychological, functional, social, and existential. The test-retest reliability (30-minute intervals) showed a weighted kappa from 0.53–1, with the majority of the items (88%) showing substantial (0.61–0.8) to almost perfect (greater than 0.8) agreement.
The symptoms are rated on a five-point Likert-type scale to assess frequency of symptoms which they encountered in the past week, ranging from 1 (never) to 5 (always), and a four-point Likert-type scale to assess intensity of the prevalent symptoms experienced in the past week, ranging from 1 (not serious) to 4 (very serious). One symptom, weight loss, receives a dichotomized answer category (0 for “yes” or 1 for “no”).
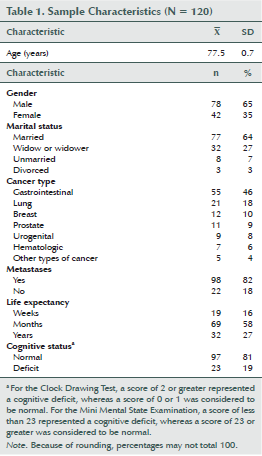
Additional demographics and clinical data were collected, including age, gender, marital status, and living status (see Table 1). Clinical data collected included cognition assessed by the Clock Drawing Test (CDT) (Shulman, Pushkar Gold, Cohen, & Zucchero, 1993) or Mini Mental State Examination (MMSE) (Tombaugh & McIntyre, 1992), life expectancy (weeks, months, years), type of malignant disease, metastases (yes or no), and Flemish Triage Risk Screening Tool (TRST) (Deschodt et al., 2011).
Data Collection
Ethical approval was obtained by the ethics review committee of the two general hospitals. Eligible patients were identified by the attending physicians. The physicians provided oral information about the study to the patient. After consent, the patients, proxies, and nurses were approached by one of the two research assistants who explained the study more extensively. Patients who agreed to participate were asked to sign an informed consent. Proxies and nurses provided oral consent.
Patients, nurses, and proxies of the patients assessed the symptoms independently on the same day using the validated instrument. Patients completed the instrument by means of a standardized and structured interview with one of the two researchers. The nurses and proxies received the instrument in hard copy.
Data Analysis
The data were analyzed using SPSS®, version 20. Descriptive statistics and symptoms were presented in absolute numbers and frequencies. The level of agreement was examined using three different methods as described by Laugsand et al. (2010). First, agreement at the individual level was measured using the Wilcoxon Signed-Rank test to compare the frequency and intensity of symptoms as assessed by the three assessors. Second, differences in scores were measured for frequency and intensity of each symptom. The difference score was computed by (a) subtracting the score of the patient from the score of the nurse and (b) subtracting the score of the patient from the score of the proxy. Patient assessment was seen as the gold standard. Difference scores (DS) were interpreted as follows: DS of ± 1, good agreement; DS of –2 or lower, underestimation; DS of 2 or greater, overestimation. Third, agreement at the individual level was measured using the intraclass correlation coefficient (ICC), two-way mixed effect model, and the absolute agreement. The ICC was reported with its 95% confidence interval (CI). The strength of agreement was interpreted according to Landis and Koch (1977): 0–0.2, poor; 0.21–0.4, fair; 0.41–0.6, moderate; 0.61–0.8, substantial; and 0.81–1, almost perfect.
The DS were used to investigate the demographic and disease-related factors associated with under- and overestimation and good agreement. The chi-square test was used to measure this association. A p value of less than 0.05 was considered significant.
Results
A total of 120 hospitalized patients participated in the study. Patients had a mean age of 77.5 years (SD = 0.7). The five most prevalent symptoms were fatigue (86%), lack of energy (84%), lack of appetite (81%), dry mouth (79%), and difficulties with self-care abilities (73%). Agreement scores of symptom assessment at group level between patients, nurses, and proxies are provided in Table 2.
[[{"type":"media","view_mode":"media_original","fid":"19621","attributes":{"alt":"","class":"media-image","height":"517","typeof":"foaf:Image","width":"723"}}]]
[[{"type":"media","view_mode":"media_original","fid":"19631","attributes":{"alt":"","class":"media-image","height":"519","typeof":"foaf:Image","width":"726"}}]]
[[{"type":"media","view_mode":"media_original","fid":"19636","attributes":{"alt":"","class":"media-image","height":"517","typeof":"foaf:Image","width":"722"}}]]
[[{"type":"media","view_mode":"media_original","fid":"19641","attributes":{"alt":"","class":"media-image","height":"516","typeof":"foaf:Image","width":"721"}}]]
[[{"type":"media","view_mode":"media_original","fid":"19646","attributes":{"alt":"","class":"media-image","height":"515","typeof":"foaf:Image","width":"724"}}]]
Nurses tended to report lower symptom frequency and intensity compared to patients; however, for 61% of the symptoms, no significant difference in agreement between patients and nurses was noted. Proxies tended to report higher symptom frequency and intensity compared to patients. However, this was not the case for all symptoms. No significant differences were noted between patients and their proxies for frequency (81%) and intensity (89%) of symptoms. The direct over- and underestimation of symptoms defined as a DS of –2 or less or 2 or greater are provided in Table 3.
The frequency of symptoms most underestimated by nurses were dry mouth (43%) and changes in the taste of food (39%). Best agreement was found for the assessment of fecal incontinence (93%), vomiting (92%), and diarrhea (92%). The intensity of symptoms most underestimated by nurses were fatigue (8%) and difficulties with self-care (8%). The frequency of the symptom most often overestimated by nurses was fear (19%). The intensity of the symptom most often overestimated by nurses was difficulties with self-care (5%).
The frequency of symptoms most underestimated by proxies were dry mouth (19%) and tingling in hands or feet (15%). Best agreement was found for feeling supported (97%), vomiting (93%), and fecal incontinence (94%). The intensity of the symptom most underestimated by proxies (anger) was 7%. The frequency of the symptoms most often overestimated by proxies were 24% (brooding), 23% (tension), 23% (nervousness), and 23% (fear). The symptom intensity most often overestimated by proxies (lack of energy) was (6%).
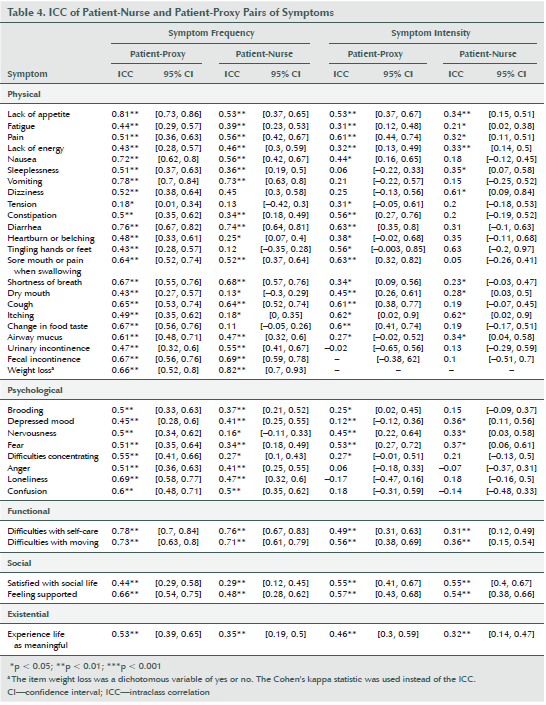
Agreement of symptoms at individual levels between patients, nurses, and proxies is provided in Table 4. Higher agreement existed concerning the frequency of symptoms compared to the intensity of symptoms. In addition, better ICCs were identified between patients and proxies compared to between patients and nurses. The agreement between patients and proxies was for the frequency of all symptoms moderate to excellent, except for the symptom of tension (ICC = 0.18). Fifteen symptoms showed poor to fair agreement between patients and nurses for frequency. Agreement on the intensity of symptoms was low for both dyads.
The 120 patients, nurses, and proxies each assessed 35 symptoms. The symptom of weight loss was not included in the analysis on factors associated with the over- and underestimation of symptoms because a DS could not be calculated for this dichotomous variable. This yielded a total of 4,200 patient-nurse and patient-proxy observations for symptom frequency. Fewer dyads (range = 1,560–1,800) were measured for symptom intensity because the latter could only be rated for prevalent symptoms.
[[{"type":"media","view_mode":"media_original","fid":"19606","attributes":{"alt":"","class":"media-image","height":"514","typeof":"foaf:Image","width":"722"}}]]
[[{"type":"media","view_mode":"media_original","fid":"19611","attributes":{"alt":"","class":"media-image","height":"515","typeof":"foaf:Image","width":"723"}}]]
[[{"type":"media","view_mode":"media_original","fid":"19616","attributes":{"alt":"","class":"media-image","height":"245","typeof":"foaf:Image","width":"725"}}]]
The agreement between patients and nurses on symptom frequency was associated with gender, marital status, living status, presence of metastases, expected prognosis, and treatment with radiation therapy (see Table 5). Nurses more often underestimated symptom frequency in female patients, patients living with both partner and other(s), and patients receiving radiation therapy. Overestimation of symptom frequency by nurses was more prevalent in male patients, divorced patients, patients living alone, and patients having metastases. The agreement between patients and nurses on symptom intensity was associated with gender, marital status, living status, cancer type, metastases, expected prognosis, and radiation therapy. Nurses more often underestimated symptom intensity in male patients, patients aged 75–79 years, patients living with both partner and/or other(s), patients with no metastases, patient with a life expectancy of years (compared to weeks and months), and patients receiving radiation therapy. Overestimation of symptom intensity by nurses was more prevalent in female patients, patients aged 70–74 years, and patients with breast cancer.
The agreement between patients and proxies on symptom frequency was associated with marital status, living status, cognitive status, cancer type, metastases, expected prognosis, and chemotherapy. Proxies more often underestimated symptom frequency in patients living with both partner and other(s), patients with impaired cognition, and patients with breast and hematologic cancers. Overestimation of symptom frequency by proxies was more prevalent in widowed patients, patients living alone and with others, patients with normal cognitive function, patients with urogenital and lung cancer, patients with no metastases, and patients treated with chemotherapy. The agreement between patients and proxies on symptom intensity was associated with gender, age, marital status, cognitive status, metastases, expected prognosis, radiation therapy, and chemotherapy. Proxies more often underestimated symptom intensity in male patients, patients aged 65–69 years, unmarried patients, patients with no metastases, patients with a life expectancy of years, and patients receiving radiation therapy. Overestimation of symptom intensity by proxies was more prevalent in female patients, patients aged 85–89 years, patients with impaired cognition, and patients not receiving chemotherapy.
Discussion
This study investigated the agreement between patients, nurses, and proxies with regard to symptom assessment. The results of this study indicate that nurses and patient proxies tend to underestimate physical and social symptoms and overestimate psychological, functional, and existential symptoms. However, agreement was for the majority (greater than 60%) of the symptoms not statistically significant (p > 0.05), which indicates that the observed differences might arise from chance only. The agreement of the frequency of symptoms between patients and proxies was better than the agreement between patients and nurses. Overall, agreement was better for less-subjective symptoms and symptoms that are less humiliating for patients to talk about (Brorsson, Lindbladh, & Rastam, 1998; Dewar, Gregg, White, & Lander, 2009). Agreement between the intensity assessment of symptoms was, for most (greater than 50%) of the symptoms, rated as poor to fair between patient and nurse and patient and proxy.
Most previous studies were conducted in a population and setting different from hospitalized older palliative patients with cancer, except for Pautex et al. (2003). The findings of the current study confirm the results of Pautex et al. (2003). However, the current study included a larger number of patients and assessed symptoms in more domains.
The findings are somewhat in contrast with a large multicenter study of adult patients with cancer (Laugsand et al., 2010). Laugsand et al. (2010) indicated that healthcare providers underestimate symptoms in about 10% of the patients, regardless of the type of symptom. However, the adult patients with cancer included in a study by Laugsand et al. (2010) differs somewhat from the older palliative patients with cancer included in the current study because the latter is more vulnerable to comorbidities, cognitive problems, and dependency. The current study measured a significant association between cognitive status and the agreement of symptom frequency and intensity between patients and proxies, indicating underestimation by proxies. This association was not significant between patients and nurses, but the absolute values suggest an underestimation by nurses. These findings are in contrast with the findings of Laugsand et al. (2010), who reported less agreement in patients with a normal cognitive status. Less agreement seems to be present in patients of younger age. However, no significant association was measured for frequency, in contrast to intensity.
Differences in scores could be the result of patient bias. In the current study, patient report was seen as the gold standard. However, one could question the true representation of the symptoms as reported by patients. Literature suggests that patients, particularly older adult patients, sometimes minimize their symptoms for a variety of reasons, such as not wanting to be a burden to others (McPherson, Wilson, Chyurlia, & Leclerc, 2010; McPherson, Wilson, & Murray, 2007), seeing symptoms as part of aging (Kaye et al., 2010), and denying symptoms as coping mechanism (Arraras, Wright, Jusue, Tejedor, & Calvo, 2002; Hauer et al., 2009).
This study has some strengths that enhance the validity of the results. First, this study is the first, to the authors’ knowledge, to measure the agreement between patients and nurses and patients and proxies regarding symptom frequency and intensity on five domains (physical, psychological, functional, social, and existential) in older palliative patients with cancer. Second, patients had to be hospitalized for at least a week to allow nurses to build a relationship with the patient and to get to know the patient. In addition, patients had to receive a visit from at least one person in the past week to enable a good estimation of the symptoms by the proxy.
This study also has some limitations. First, no demographic information was gathered for the nurses and proxies. The collection of this data would have allowed the authors to identify if certain variables at nurse and proxy level could have explained under- or overestimation of symptoms. Bahrami, Parker, and Blackman (2008) reported that the clinical experience of an oncology nurse was a significant predictor of agreement between patients and nurses. Higginson and Gao (2008) reported that higher caregiver burden was significantly associated with agreement on symptom assessment. Second, the study was a cross-sectional study, which does not allow for the identification of a causal relationship. Third, generalization of the results could be limited because the study was performed in two non-randomly selected general hospitals in Belgium.
Implications for Nursing and Research
The results of this study indicate that proxies are somewhat better than nurses in estimating the symptoms that patients experience. However, the findings raise some concerns when treatment options and decisions are based on the estimation of symptoms made by nurses and proxies. The general underestimation of physical and social symptoms and overestimation of psychological, functional, and existential symptoms could result in under- and overtreatment. Undertreatment could lead to needless discomfort and decreased quality of life. In palliative care, overtreatment in terms of receiving holistic attention could be judged as unharmful. However, overtreatment in terms of higher doses of medication could have side effects, and painful interventions are equivalent to undertreatment.
[[{"type":"media","view_mode":"media_original","fid":"19651","attributes":{"alt":"","class":"media-image","height":"516","typeof":"foaf:Image","width":"726"}}]]
[[{"type":"media","view_mode":"media_original","fid":"19656","attributes":{"alt":"","class":"media-image","height":"516","typeof":"foaf:Image","width":"723"}}]]
[[{"type":"media","view_mode":"media_original","fid":"19661","attributes":{"alt":"","class":"media-image","height":"515","typeof":"foaf:Image","width":"723"}}]]
As a result of the differences in assessment between patients, nurses, and proxies, it is advised to combine patient-, nurse-, and proxy-reported symptom assessment in clinical practice and research. Treatment decisions should be based on this combined evaluation to optimize care. However, in clinical practice, symptoms often are assessed by one party only. Patients should be encouraged to report their true experience, and misconceptions should be addressed through education. Nurses and proxies should be taught to recognize and assess symptoms and to communicate about it with patients. The literature implies that patients do not always report their true experiences, but strong evidence is lacking to support that implication. More research is needed on the reasons for symptom disagreements between patients, nurses, and proxies. This can be achieved by research focusing on (a) reasons why patients do or do not report their symptoms, (b) how nurses and proxies recognize and assess symptoms, and (c) the underlying thoughts of patients, nurses, and proxies regarding the report and assessment of symptoms. Those insights will provide indications to set up interventions to improve symptom assessment and symptom agreement.
[[{"type":"media","view_mode":"media_original","fid":"19601","attributes":{"alt":"","class":"media-image","height":"220","typeof":"foaf:Image","width":"367"}}]]
Conclusion
The current study indicates that nurses and proxies tend to underestimate physical and social symptoms and overestimate psychological, functional, and existential symptoms. Agreement was associated with multiple demographic and clinical factors, such as gender and presence or absence of metastases. Treatment interventions should be based on a combined assessment of symptoms by the patient, a healthcare professional, and the patients’ proxies. More insight is needed in reasons of disagreement on symptoms between patients, nurses, and proxies. These insights will provide indications to set up interventions to improve symptom assessment and symptom agreement.
References
Arraras, J.I., Wright, S.J., Jusue, G., Tejedor, M., & Calvo, J.I. (2002). Coping style, locus of control, psychological distress and pain-related behaviours in cancer and other diseases. Psychology, Health and Medicine, 7, 181–187. doi:10.1080/13548500120116139
Bahrami, M., Parker, S., & Blackman, I. (2008). Patients’ quality of life: A comparison of patient and nurse perceptions. Contemporary Nurse, 29, 67–79. doi:10.5172/conu.673.29.1.67
Brorsson, A., Lindbladh, E., & Rastam, L. (1998). Fears of disease and disability in elderly primary health care patients. Patient Education and Counseling, 34, 75–81. doi:10.1016/S0738-3991(98)00052-4
Depp, C.A., & Jeste, D.V. (2006). Definitions and predictors of successful aging: a comprehensive review of larger quantitative studies. American Journal of Geriatric Psychiatry, 14, 6–20. doi:10.1097/01.JGP.0000192501.03069.bc
Deschodt, M., Wellens, N.I.H., Braes, T., De Vuyst, A., Boonen, S., Flamaing, J., . . . Milisen, K. (2011). Prediction of functional decline in older hospitalized patients: A comparative multicenter study of three screening tools. Aging Clinical and Experimental Research, 23(5–6), 421–426. doi:10.1007/BF03325237
Desmedt, M.S., de la Kethulle, Y.L., Deveugele, M.I., Keirse, E.A., Paulus, D.J., Menten, J.J., . . . Beguin, C.M. (2011). Palliative inpatients in general hospitals: a one day observational study in Belgium. BMC Palliative Care, 10, 2. doi:10.1186/1472-684X-10-2
Dewar, A., Gregg, K., White, M., & Lander, J. (2009). Navigating the health care system: Perceptions of patients with chronic pain. Chronic Diseases in Canada, 29(4), 162–168.
Ferlay, J., Shin, H.R., Bray, F., Forman, D., Mathers, C., & Parkin, D.M. (2010). Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. International Journal of Cancer, 127, 2893. doi:10.1002/ijc.25516
Hauer, K., Tremmel, A.D., Ramroth, H., Pfisterer, M., Todd, C., Oster, P., & Schuler, M. (2009). Repressive coping in geriatric patients’ reports–Impact on fear of falling. Zeitschrift für Gerontologie und Geriatrie, 42, 137–144. doi:10.1007/s00391-008-0552-9
Higginson, I.J., & Gao, W. (2008). Caregiver assessment of patients with advanced cancer: Concordance with patients, effect of burden and positivity. Health and Quality of Life Outcomes, 6, 42. doi:10.1186/1477-7525-6-42
Kaye, A.D., Baluch, A., & Scott, J.T. (2010). Pain management in the elderly population: A review. Ochsner Journal, 10(3), 179–187.
Landis, J.R., & Koch, G.G. (1977). The measurement of observer agreement for categorical data. Biometrics, 33, 159–174. doi:10.2307/2 529310
Laugsand, E.A., Sprangers, M.A., Bjordal, K., Skorpen, F., Kaasa, S., & Klepstad, P. (2010). Health care providers underestimate symptom intensities of cancer patients: A multicenter European study. Health Quality of Life Outcomes, 8, 104. doi:10.1186/1477-7525-8-104
Lynn, M.R. (1986). Determination and quantification of content validity. Nursing Research, 35, 382–385.
Marengoni, A., Angleman, S., Melis, R., Mangialasche, F., Karp, A., Garmen, A., . . . Fratiglioni, L. (2011). Aging with multimorbidity: A systematic review of the literature. Ageing Research Reviews, 10, 430–439. doi:10.1016/j.arr.2011.03.003
McPherson, C.J., Wilson, K.G., Chyurlia, L., & Leclerc, C. (2010). The balance of give and take in caregiver–partner relationships: An examination of self-perceived burden, relationship equity, and quality of life from the perspective of care recipients following stroke. Rehabilitation Psychology, 55, 194. doi:10.1037/a0019359
McPherson, C.J., Wilson, K.G., & Murray, M.A. (2007). Feeling like a burden to others: A systematic review focusing on the end of life. Palliative Medicine, 21, 115–128. doi:10.1177/0269216307076345
Nekolaichuk, C.L., Bruera, E., Spachynski, K., MacEachern, T., Hanson, J., & Maguire, T.O. (1999). A comparison of patient and proxy symptom assessments in advanced cancer patients. Palliative Medicine, 13, 311–323.
Pautex, S., Berger, A., Chatelain, C., Herrmann, F., & Zulian, G.B. (2003). Symptom assessment in elderly cancer patients receiving palliative care. Critical Review in Oncology/Hematology, 47, 281–286. doi:10.1016/S1040-8428(03)00043-X
Polit, D.F., & Beck, C.T. (2011). Nursing research. Generating and assessing rvidence for nursing practice (9th ed.). New York, NY: Lippincott Williams and Wilkins.
Shulman, K.I., Pushkar Gold, D., Cohen, C.A., & Zucchero, C.A. (1993). Clock-drawing and dementia in the community: A longitudinal study. International Journal of Geriatric Psychiatry, 8, 487–496. doi:10.1002/gps.930080606
Teunissen, S.C., Wesker, W., Kruitwagen, C., de Haes, H.C., Voest, E.E., & de Graeff, A. (2007). Symptom prevalence in patients with incurable cancer: A systematic review. Journal of Pain and Symptom Management, 34, 94–104. doi:10.1016/j.jpainsymman.2006.10.015
Tombaugh, T.N., & McIntyre, N.J. (1992). The Mini-Mental State Examination: A comprehensive review. Journal of the American Geriatrics Society, 40, 922–935.
Van Lancker, A., Beeckman, D., Van Den Noortgate, N., Grypdonck, M., Van Hecke, A., & Verhaeghe, S. (2012). [The prevalence and control of symptoms in elderly with incurable cancer: Instrument development and validation]. Abstract presented at Vlaams-Nederlands Onderzoeksforum Palliatieve Zorg.
Van Lancker, A., Velghe, A., Van Hecke, A., Verbrugghe, M., Van Den Noortgate, N., Grypdonck, M., . . . Beeckman, D. (2014). Prevalence of symptoms in older palliative cancer patients: A systematic review and meta-analysis. Journal of Pain and Symptom Management, 47, 90–104. doi:10.1016/j.jpainsymman.2013.02.016
Winn, P.A.S., & Dentino, A.N. (2005). Quality palliative care in long-term care settings. Journal of the American Medical Directors Association, 6, 197–206. doi:10.1016/j.jamda.2005.03.019
World Health Organization. (2002). National cancer control programmes: Policies and managerial guidelines (2nd ed.). Geneva, Switzerland: Author.
Yip, J.Y., Wilber, K.H., Myrtle, R.C., & Grazman, D.N. (2001). Comparison of older adult subject and proxy responses on the SF-36 health-related quality of life instrument. Aging and Mental Health, 5, 136–142. doi:10.1080/13607860120038357