Providing Palliative Care: Oncology Nurses’ Perceptions of Their Self-Reported Abilities
Background: Oncology nurses are pivotal in the provision of primary palliative care. However, nurses working in oncology settings, where the goal is often curative, may lack knowledge about and comfort in providing palliative care.
Objectives: The purpose of this study is to determine how oncology nurses perceive their ability to provide palliative care services to patients and their families.
Methods: Using Benner’s theory of skill acquisition as a basis for self-evaluation, this cross-sectional, descriptive pilot study surveyed oncology nurses.
Findings: All participants reported ranges from capable to very capable in ability to provide precepts of palliative care. Results showed a small but statistically significant association between years of experience and perceived ability to honor patient and family preferences, provide patient and family support, appreciate demands placed on families, and provide supportive services to caregivers.
Jump to a section
Receiving a cancer diagnosis is a life-altering experience, broadly affecting individuals and their family members as they adapt to and cope with physical symptoms, such as pain, and the emotional burdens of uncertainty and fear. The Oncology Nursing Society (2019) and the National Comprehensive Cancer Network (2019) recommend that an interprofessional team deliver comprehensive, patient- and family-centered palliative care starting at diagnosis, concurrent with treatment, and continuing throughout the cancer journey, including survivorship. Therefore, oncology nurses, as members of the interprofessional team, are pivotal to providing primary palliative care, including direct care, care coordination, and patient and family advocacy and education (National Coalition for Hospice and Palliative Care, 2018). Palliative care, an approach for caring for patients who are facing life-threatening illness and their families, aims to improve quality of life “through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual” (World Health Organization, 2019, para. 1). Palliative care is a holistic approach to care that may benefit all people affected by a cancer diagnosis, including patients’ families and caregivers (National Cancer Institute, 2017).
Despite the ongoing support from national bodies and professional organizations, and the widespread availability of guidelines and resources, the adoption of palliative care remains limited. To support and expand palliative care, the National Academies of Sciences, Engineering, and Medicine (formerly known as the Institute of Medicine [IOM], 2015) supports a national strategy to improve access to palliative care and improve healthcare workforce training. That training includes building skills in pain and symptom management and care coordination (IOM, 2015; Meier et al., 2017).
Background
As a complement to clinical oncology care, nurses who provide palliative care are confident in their abilities and can advocate for patients. Few studies have identified nurses’ ability to provide palliative care. Therefore, there is a lack of studies about palliative care education in clinical oncology settings. An integrative review by Achora and Labrague (2019) about nurses’ knowledge about and attitudes toward providing palliative care in a variety of settings suggested that nurses have positive attitudes toward palliative care, despite a general lack of knowledge—specifically, knowledge related to pain and symptom management, psychological care, and philosophies of palliative care delivery.
The purpose of this pilot study is to determine how oncology nurses perceive their ability to provide elements of primary palliative care to patients and their families. In addition, related to palliative care competencies, this study explores the relationship between participants’ self-reported perception of ability to provide precepts of palliative care, years of experience, and highest level of education.
Methods
This was a cross-sectional, descriptive pilot study of oncology nurses practicing at the Roswell Park Comprehensive Cancer Center in Buffalo, New York. The institute provides comprehensive cancer care to the region and has a palliative care team available for consultation.
Sample
A convenience sample of oncology nurses was obtained from a recruitment letter sent via the cancer institute’s email system, which invited potential participants to follow a link to an online survey on SurveyMonkey®. Data were collected during a four-week period after obtaining approval from the institutional review board at the cancer center and Daemen College in Amherst, New York. Seventy-nine nurses self-selected to voluntarily participate in the study.
Measurement
To document the study sample’s demographics, study participants provided their highest level of education and years of experience. The study survey was based on four of the five precepts of palliative care. The precepts guide nursing care and are foundational to clinical practice guidelines. The precepts use eight declarative statements (S1–S8) (National Coalition for Hospice and Palliative Care, 2018; Task Force on Palliative Care, Last Acts Campaign, & Robert Wood Johnson Foundation, 1998) (see Table 1). Precepts 1–4 focus on nurses’ perceived abilities at the bedside. Precept 5 was not included in the survey because it is related to organizational infrastructure. 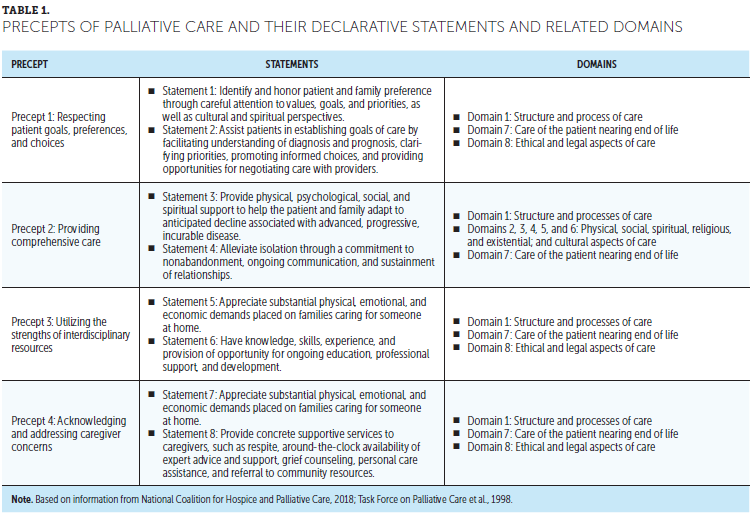
Using Benner’s (2001) novice to expert categories, for each of the eight statements, participants ranked their perceived ability to provide the precepts (on a Likert-type scale ranging from 1 [novice] to 5 [expert]). The five stages of skill development in nursing are as follows (Benner, 2001):
• Novice: those without any experience
• Advanced beginner: able to guide actions based on rules and experiences
• Competent: some feelings of mastery based on experience, which serve as guidelines to plan care
• Proficient: ability to view situations as a whole because they have multiple perspectives on the situation
• Expert: inherent intuitive grasp formed through a deep understanding of the situation
When adapting Benner’s (2001) theory of skill acquisition, both novice and expert remained ranked as defined by Benner. A participant who indicated feeling somewhat capable was considered equivalent to an advanced beginner, capable was considered to be competent, and very capable was deemed proficient.
Analysis
Descriptive statistics were used to evaluate data collected using IBM SPSS Statistics, version 25.0. Analysis of variance (ANOVA) determined whether there was a statistically significant difference between highest level of education and years of experience, and highest level of education and responses to the eight statements on the precepts (S1–S8). Likert-type responses, from 1 (novice) to 5 (expert), were treated as a continuous variable. In addition, the Student–Newman–Keuls stepwise multiple comparisons procedure was used as a secondary test to determine statistical significance (i.e., risk of a false-positive result) (p < 0.05). Correlations, which measure the strength and direction of the relationship, ranging from +1 to –1, between highest level of education and each precept (S1–S8) are reported using Spearman’s rho. Correlations between years of nursing experience and precepts (S1–S8) are reported using Spearman’s rho and Pearson’s r. Pearson’s r is used to measure the relationship between two continuous variables, and Spearman’s rho evaluates continuous or ordinal-level variables. The strength of correlation for both approaches are considered to be small (0.1 to 0.2), medium (0.3 to 0.4), and large (0.5 to 1) (Polit & Beck, 2014).
Findings
Seventy-nine oncology nurses participated in the study. The majority of the participants (n = 51) had more than 10 years of experience, and 10 participants had fewer than 5 years of experience; one participant chose not to report experience (see Table 2). Based on 2017 benchmarks, the National Council of State Boards of Nursing (2019) established that 42% of nurses had a bachelor’s degree as qualification for first license. Of the study participants, 36 (46%) had earned a bachelor’s degree and 13 (16%) had earned a master’s degree. 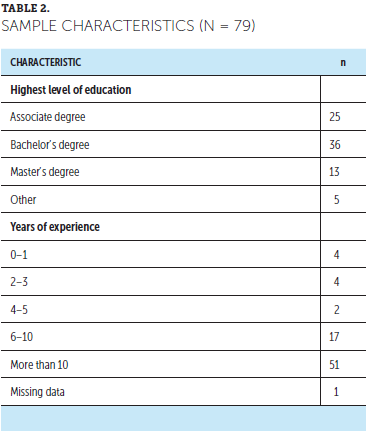
Perceptions of Ability to Provide Precepts of Palliative Care
The majority of the participants reported their ability to provide the precepts in the range of capable to very capable for all eight statements (see Table 3). Honoring preferences (S1) was the highest-ranked item, with 57 respondents indicating that they perceived themselves to be very capable and 7 considering themselves to be expert (mean = 3.9, SD = 0.59). This statement (S1) supports participants’ perceived ability to identify and honor preferences of patients and families through careful attention to their values, goals, and priorities, as well as their cultural and spiritual perspectives. In addition, demands placed on families (S7, precept 4) indicated that 44 oncology nurses perceived themselves as being very capable and 17 as being experts in their ability to appreciate the substantial physical, emotional, and economic demands placed on families (mean = 3.9, SD = 0.75). This statement (S7) relates to the participants’ ability to acknowledge and address caregiver concerns. 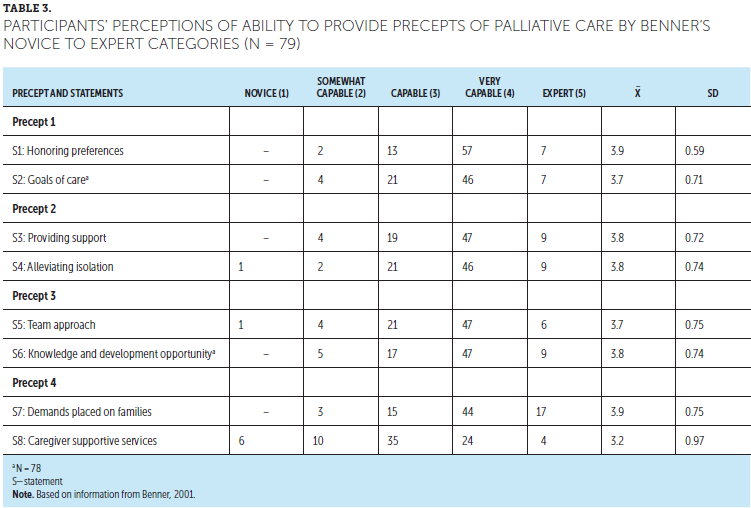
Years of Nursing Experience by Highest Level of Education
There was no statistical difference in the sample between highest level of education and years of experience, except for participants without an academic degree. Five respondents had, on average, 27.2 years of experience but did not indicate having a conferred associate, bachelor’s, or master’s degree (see Tables 4 and 5). 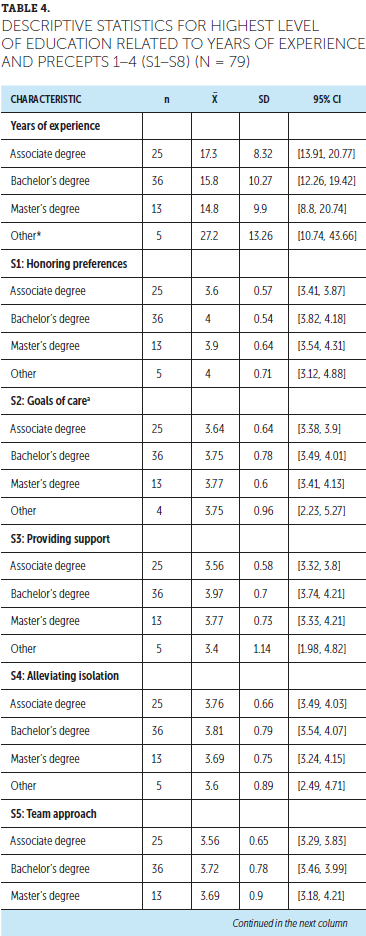
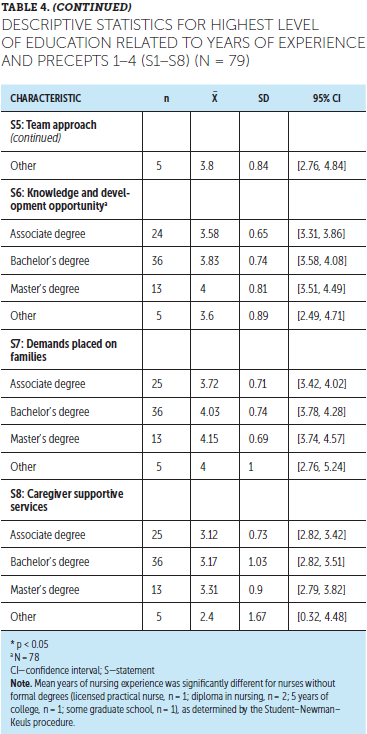
Perception of Ability
There was a small but statistically significant positive correlation between years of nursing experience and honoring preferences (S1) (r = 0.23), providing support (S3) (r = 0.28), demands placed on families (S7) (r = 0.14, p < 0.05), and caregiver supportive services (S8) (r = 0.3, p < 0.01). Years of nursing experience and knowledge and development opportunity (S6) were near statistical significance (r = 0.28, p = 0.06), which suggests that there may be an effect but not enough of one to reject the null hypothesis. Universally, caregiver supportive services (S8) was the weakest perceived ability reported. There was a medium positive correlation between years of experience and caregiver supportive services (S8) (r = 0.31, p < 0.01) (see Table 6). However, there was no statistically significant correlation between highest level of education and S1–S8. 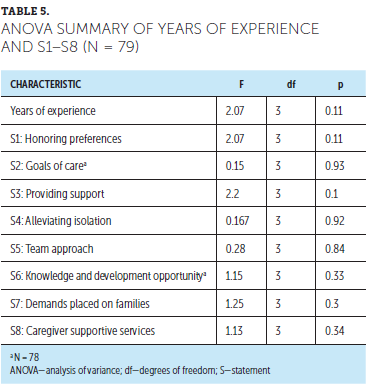
Discussion
This pilot study reports on the perceived ability of oncology nurses to deliver the precepts of palliative care at a large urban inpatient cancer institute in New York. Overall, oncology nurses reported that they had a strong ability to provide the precepts; this finding supports the current clinical practice guidelines to deliver palliative care as an interprofessional team (National Coalition for Hospice and Palliative Care, 2018). This study revealed that years of nursing experience correlates with precepts of palliative care in several areas; however, highest level of education was not associated with any of the precepts. These findings suggest that, although nurses may perceive themselves as being proficient, this is not necessarily a product of years of formal education, but rather from experience or specific training in palliative care. Benner (2001) stated that the number of years of nursing experience in the same work environment, and in the same or similar medical situations, can establish and build competence in nurses’ clinical practice. As revealed in this pilot study’s results, nurses with additional years of experience perceived their abilities as higher than their less experienced counterparts. In addition, these findings may also be influenced by exposure to, and interactions with, the palliative care consultation team. [[{"fid":"54151","view_mode":"default","fields":{"format":"default","alignment":"","field_file_image_alt_text[und][0][value]":false,"field_file_image_title_text[und][0][value]":false},"link_text":null,"type":"media","field_deltas":{"2":{"format":"default","alignment":"","field_file_image_alt_text[und][0][value]":false,"field_file_image_title_text[und][0][value]":false}},"attributes":{"class":"media-element file-default","data-delta":"2"}}]]
This pilot study’s findings support the findings from previous studies about nurses’ years of experience and their perceptions of their ability to provide palliative and end-of-life care. For example, Price et al. (2017) reported that nurses with more than 10 years of experience working in intensive care perceived themselves to be more competent in providing end-of-life care, scoring higher knowledge, decision making, emotional support for family, and spiritual support competencies than nurses with fewer than 10 years of experience. In the current study, the majority of participants had more than 10 years of experience and reported themselves as being capable or very capable in their ability to perform precepts of palliative care, as measured in S1–S7.
The lowest mean score for perceived ability was in precept 4, caregiver supportive services (S8); however, this statement was most highly correlated with years of nursing experience, suggesting that more experienced nurses are more comfortable in providing support to patients and their families. In addition, nurses who practice in oncology settings are highly attuned to meeting the physical and emotional needs of patients with cancer, regardless of whether they are receiving palliative care services, in contrast to nurses in general practice who identify having poor knowledge of approaches for pain and symptom management (Achora & Labrague, 2019). Therefore, this may have an impact on the participants’ report of expertise in precept 2, which is related to the physical and emotional demands of patients.
Limitations
Pilot study participants volunteered to participate in the study and provided self-reported perceptions. This could influence the results because of self-selection and variations in personal practice patterns. In addition, the small sample size limits generalizability to inpatient oncology settings. The evaluation tool was developed by the researchers, and it has not been validated. This pilot study did not address a complete set of clinical practice guidelines because the study focused on selected precepts of palliative care.
In addition, the “other” group in years of experience combined a small sample of individuals with conceptually unrelated levels of experience, which could affect the findings of this pilot study. There is also a wide 95% confidence interval in this domain, which reduces the certainty of the finding. However, it was necessary to group these individuals together for analysis because there were only five participants without a traditional nursing education.
Implications for Practice
Based on this pilot study’s findings, nurses with more than 10 years of experience, who are defined as experts in Benner’s (2001) model, may act as guides and facilitators for novice and advanced beginners in nursing who are learning how to provide palliative care. Clinical oncology nurses have the expertise to manage patients with cancer, supporting them and their family members during the trajectory of what may be incurable disease. This expertise includes delivering palliative care. However, nurses may not have the confidence and experience related to caregiver supportive services (S8, precept 4). These findings emphasize the importance of education for nurses in practice and students in nursing programs so that they can improve their abilities and confidence in supporting patients’ families. Initiatives that support palliative care nurse education can significantly affect nurses’ foundational knowledge about palliative care, as well as their attitudes toward and behaviors in better delivering that care (Harden, Price, Duffy, Galunas, & Rodgers, 2017).
This study’s findings endorse the call from the American Association of Colleges of Nursing’s new competencies and recommendations for educating undergraduate nursing students, which urge nurse educators to implement 17 palliative care competencies in undergraduate curricula (Ferrell, Malloy, Mazanec, & Virani, 2016). Several of these nursing competencies are family-centered, including educating family about palliative care issues (competency 5); collaborating with members of the interprofessional team, specifically aimed at ensuring coordinated care (competency 6); assisting the family to cope and build resilience (competency 16); and recognizing the need to seek consultation (competency 17) (Ferrell et al., 2016).
The current study also supports palliative care delivered by interprofessional teams, particularly to address caregiver needs. To advance interprofessional team care, experienced nurses can champion innovative methods to build competencies among team members beyond formal education programs. These methods may include focused mentorship and simulations. 
Conclusion
Based on this pilot study’s findings, oncology nurses consistently have opportunities to develop their skills in primary palliative nursing; these skills are gained through time and experience caring for patients with serious illness and their families. Engaging oncology nurses, particularly those with more than 10 years of experience—in mentorship, preceptor, and other roles in nursing education—may help bolster comfort and competence in providing palliative care. As members of interprofessional palliative care teams, experienced nurses can provide care to caregivers, ensuring that they have access to supportive services. [[{"fid":"54111","view_mode":"default","fields":{"format":"default","alignment":"","field_file_image_alt_text[und][0][value]":false,"field_file_image_title_text[und][0][value]":false},"link_text":null,"type":"media","field_deltas":{"1":{"format":"default","alignment":"","field_file_image_alt_text[und][0][value]":false,"field_file_image_title_text[und][0][value]":false}},"attributes":{"class":"media-element file-default","data-delta":"1"}}]]
About the Author(s)
Catherine M. Mann, EdD, RN, CNS, CNE, is the assistant dean of undergraduate studies and a clinical associate professor of nursing in the School of Nursing at the University of Buffalo in New York; Fatimah Rashed Aldossary, MS, RN, BS, is the postgraduate oncology nursing diploma program director at King Fahad Specialist Hospital-Dammam in Saudi Arabia; and Suzanne S. Sullivan, PhD, MBA, RN, CHPN, is an assistant professor in the School of Nursing at the University of Buffalo. The authors take full responsibility for this content and did not receive honoraria or disclose any relevant financial relationships. The article has been reviewed by independent peer reviewers to ensure that it is objective and free from bias. Mann can be reached at cmmann@buffalo.edu, with copy to CJONEditor@ons.org. (Submitted April 2019. Accepted June 13, 2019.)
References
Achora, S., & Labrague, L.J. (2019). An integrative review on knowledge and attitudes of nurses toward palliative care: Implications for practice. Journal of Hospice and Palliative Nursing, 21, 29–37. https://doi.org/10.1097/NJH.0000000000000481
Benner, P.E. (2001). From novice to expert: Excellence and power in clinical nursing practice (Commemorative ed.). Upper Saddle River, NJ: Prentice Hall.
Ferrell, B., Malloy, P., Mazanec, P., & Virani, R. (2016). CARES: AACN’s new competencies and recommendations for educating undergraduate nursing students to improve palliative care. Journal of Professional Nursing, 32, 327–333. https://doi.org/10.1016/j.profnurs.2016.07.002
Harden, K., Price, D., Duffy, E., Galunas, L., & Rodgers, C. (2017). Palliative care: Improving nursing knowledge, attitudes, and behaviors [Online exclusive]. Clinical Journal of Oncology Nursing, 21, E232–E238. https://doi.org/10.188/17CJON.E232-E238
Institute of Medicine. (2015). Dying in America: Improving quality and honoring individual preferences near the end of life. Washington, DC: National Academies Press.
Meier, D.E., Back, A.L., Berman, A., Block, S.D., Corrigan, J.M., & Morrison, R.S. (2017). A national strategy for palliative care. Health Affairs, 36, 1265–1273. https://doi.org/10.1377/hlthaff.2017.0164
National Cancer Institute. (2017). Palliative care in cancer. Retrieved from https://www.cancer.gov/about-cancer/advanced-cancer/care-choices/pallia…
National Coalition for Hospice and Palliative Care. (2018). Clinical practice guidelines for quality palliative care (4th ed.). Richmond, VA: Author.
National Comprehensive Cancer Network. (2019). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Palliative care [v.2.2019]. Retrieved from https://www.nccn.org/professionals/physician_gls/PDF/palliative.pdf
National Council of State Boards of Nursing. (2019). National nursing workforce study. Retrieved from https://www.ncsbn.org/workforce.htm
Oncology Nursing Society. (2019). Palliative care for people with cancer. Retrieved from https://www.ons.org/make-difference/ons-center-advocacy-and-health-poli…
Polit, D.F., & Beck, C.T. (2014). Essentials of nursing research: Appraising evidence for nursing practice (8th ed.). Philadelphia, PA: Wolters Kluwer.
Price, D.M., Strodtman, L., Montagnini, M., Smith, H.M., Miller, J., Zybert, J., . . . Ghosh, B. (2017). Palliative and end-of-life care education needs of nurses across inpatient care settings. Journal of Continuing Education in Nursing, 48, 329–336.
Task Force on Palliative Care, Last Acts Campaign, & Robert Wood Johnson Foundation. (1998). Precepts of palliative care. Journal of Palliative Medicine, 1, 109–112. https://doi.org/10.1089/jpm.1998.1.109
World Health Organization. (2019). WHO definition of palliative care. Retrieved from https://www.who.int/cancer/palliative/definition/en


