Optune®: Practical Nursing Applications
Background: After receiving U.S. Food and Drug Administration approval for the treatment of newly diagnosed glioblastoma (GBM) in 2015, following initial approval for treatment of recurrent GBM in 2011, Optune®, a device that uses tumor-treating fields (TTFields) therapy, continues to gain acceptance in the practice environment.
Objectives: This article reviews how TTFields differ from traditional GBM treatment approaches and discusses the pivotal role nurses play in helping patients successfully use this therapy. This includes the importance of adherence to daily continuous therapy because adherence optimizes patient outcomes.
Methods: This article provides oncology nurses with practical guidance to share with patients who are candidates for treatment with TTFields, as well as information to facilitate patients’ understanding of the use of Optune and how best to incorporate it into their activities of daily living.
Findings: Nurses are key members of the multidisciplinary treatment team that manages patients with GBM. Therefore, oncology nurses are well equipped to educate patients and caregivers about the use of and benefits of adherence to TTFields.
Jump to a section
The U.S. Food and Drug Administration (FDA) approved Optune® for the treatment of newly diagnosed glioblastoma (GBM) in combination with temozolomide (TMZ) (Temodar®) in October 2015. This indication followed initial FDA approval in 2011 for treatment of recurrent GBM as a monotherapy, after histologically or radiologically confirmed recurrence in the brain postchemotherapy, and after surgical and radiation options have been exhausted (Novocure, 2015). As clinicians increasingly prescribe Optune, they must recognize the unique characteristics that comprise this innovative therapy. Understanding and anticipating the physical, emotional, and psychosocial needs of patients on tumor-treating fields (TTFields) will enable the nurse to provide the support necessary for an easier integration into the patient’s lifestyle. As TTFields have transitioned from experimental to standard therapy, nurses play a pivotal role in supporting patients and their caregivers.
Optune is a portable device that delivers alternating electric fields, termed TTFields. Transducer arrays with insulated ceramic discs are connected to the device and strategically placed on the patient’s head to deliver the treatment. Optune consists of an electric field generator, a rechargeable battery pack, a power supply, and disposable ceramic discs, or arrays. Novocure filed with the FDA for approval of second-generation Optune, which was granted on July 13, 2016. The second-generation system is about 50% lighter at 2.7 pounds and has many advanced features to facilitate convenience of portability (see Figure 1). 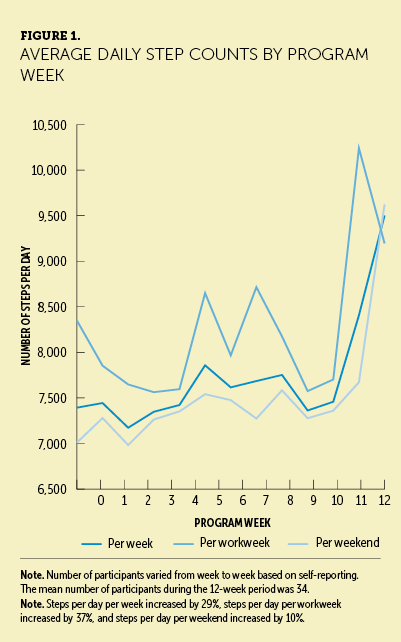
Optune has two power sources: outlet and battery power. Novocure provides a custom bag to carry the device. Patients may need assistance to adjust the carrier bag to accommodate any secondary gait impairments or muscle weakness from GBM. The desired activity level will need to be assessed by patients and caregivers to plan for therapy. Patients who prefer a high level of activity will need to plan for battery-powered operation, which requires use of the bag provided for mobile use. A fully charged battery allows for about three hours of treatment. TTFields are delivered by four transducer arrays (four sets of nine electrodes each) placed on a patient’s shaved scalp that are attached to the electric field generator, which generates 200 kHz electric fields within the brain. These patients will need to ensure that the device not only has enough battery power, but also can be worn in a functional way. Patients often become creative in incorporating TTFields into their lifestyles to minimize restrictions.
Patient Selection
Patients with primary brain tumors are a demographically and socially diverse group. An important factor in considering whether to initiate TTFields therapy is adequate support for home treatment. Optimally, patients should have at least one support person who has the capability to understand device operation, respond to alarms, report any device malfunctions or adverse events, and manage accurate array placement. Patients with poor performance status or cognitive impairment and who lack competent caregivers may be more likely to fail to adjust to TTFields treatment. Clinical trial results have demonstrated that compliance is a crucial factor in the efficacy of TTFields. Patients who were able to wear the device for a minimum of 18 hours per day for a duration of three to six months were more likely to experience a survival benefit than those who were less compliant (Mrugala et al., 2014; Stupp et al., 2012). Therefore, patient and family motivation and capabilities should be evaluated at the onset of treatment to avoid compliance issues and therapy discontinuation.
Initial Presentation
When patients are first presented with the option of being treated with TTFields, patient and family involvement is a greater consideration than when discussing traditional therapies. Adapting to this novel approach requires considerable modification in a patient’s lifestyle as compared to use of oral medication or IV treatment. Optune necessitates daily attention to device function and evaluation of proper array adherence. Because TTFields therapy requires ongoing head shaving with every array change, some patients may be reluctant to shave any hair that remains after craniotomy, radiation, and chemotherapy. Although wigs and head coverings may be worn over Optune, wearing conspicuous arrays on a shaved head with protruding wires may contribute to a feeling of self-consciousness. It is important to present the pros and cons of TTFields therapy with compassion and patience, creating an environment where patients are fully informed about the device and are at ease with their decision to implement therapy. Device support specialists (DSSs) provided by Novocure are trained to assist patients and their families with the daily operation. In addition, a 24-hour technical support hotline is provided for any other additional device concerns.
Because the lives of patients with GBM have been radically disrupted since their diagnosis, healthcare providers must allow patients and their families time to internalize the new situation and adjust to changes in daily living needed for TTFields therapy. Overcoming the unfamiliarity of TTFields cannot be sufficiently emphasized. Patients may be wary of any treatment that is not traditional surgery or chemotherapy and may find TTFields therapy to be unfamiliar. Healthcare providers should present Optune to patients as an innovative therapeutic approach with strong quality of life and survival data.
Healthcare providers should emphasize that, unlike chemotherapy, TTFields is a regional therapy that spares patients from further exacerbation of systemic side effects, such as bone marrow failure and gastrointestinal adverse events. In clinical trials, minimal adverse events were attributed to Optune (Stupp et al., 2012). Patients on TTFields may be concurrently prescribed TMZ or other FDA-approved chemotherapy drugs by their oncologists. In addition, TTFields therapy empowers patients to actively participate in their own treatment. Although the nuances of incorporating TTFields into a patient’s lifestyle may seem daunting, it puts therapeutic control back into the hands of the patient. Patients and their caregivers decide active treatment time and how to incorporate other priorities into their lifestyle.
Although identifying key priorities and goals of care is important, healthcare providers must emphasize that, during treatment with Optune, patients may continue to make activities, such as jogging, gardening, traveling, or work, a part of their daily experience. Patients who would like to continue to work may find an additional power supply or battery charger at their office helpful to minimize frustrations or barriers to use. Alternatively, a patient who wishes to keep up an exercise regimen may need additional arrays for more frequent array placement. Additional supplies are always available to the patient in an effort to facilitate compliance.
Education on the benefits of compliance helps patients and caregivers balance individual goals and schedules while optimizing the chance of extended survival. Unlike chemotherapy, TTFields have no half-life and are only effective if treatment is actively ongoing. The mechanism of action of TTFields is anti-mitotic, where alternating electric fields disrupt rapidly dividing tumor cells from undergoing division into two normal daughter cells. TTFields selectively target only actively dividing cells, and nondividing cells are not affected. Because cells divide at random, having therapy activated at least 75% of the time ensures a maximal proportion of cells undergoing mitosis will be susceptible to the effects of TTFields. Unlike checkpoint inhibitors or anti-angiogenesis drugs, preclinical data suggest that TTFields might continue to target neoplastic mitotic division for hours or days after being active, but not for weeks or months (Lee, Wong, & Swanson, 2011; Rulseh et al., 2012). Dividing malignant cells are targeted by TTFields delivering a specific electric field intensity and frequency, but not by biochemical means, so maximizing the duration of TTFields for them to attack and disrupt exponential growth of the tumor is important (Gera et al., 2015).
Clinical trials have demonstrated that patients with GBM who have attained an adherence rate of 75% daily (at least 18 of 24 hours per day) for nine months show better radiographic improvement (Mrugala et al., 2014; Stupp et al., 2012). Several possibilities can explain the reduction of overall tumor volume. TTFields might be additive or synergistic to other treatments in managing GBM growth, as evidenced in preclinical experiments (Kirson et al., 2009). The recruitment of immune mechanisms that exhibit anti-neoplastic surveillance may also play a role (Wong, Lok, Gautam, & Swanson, 2015). Although TTFields actively target rapidly dividing tumor cells, other cellular mechanisms might be working to eliminate dormant infiltrative cells.
A retrospective analysis has demonstrated that patients who were administered less than 4.1 mg of dexamethasone daily while undergoing TTFields therapy had a statistically significant improved overall survival (Wong et al., 2015). The results indirectly suggest that patients administered a lower dose of an immunosuppressive agent, such as a steroid, might be better equipped to harness natural cancer-fighting mechanisms.
Treatment Initiation
Preclinical work has demonstrated that, as electric field intensity increases, viable cell count decreases (Kirson et al., 2009). By personalizing the placement of transducer arrays, the intensity of the electric field to the region of tumor is optimized (Chaudhry et al., 2015; Kirson et al., 2009; Optune, 2016). Maximizing the intensity of the electric field to the region of tumor requires individualized mapping for each patient. Those involved in the patient’s care receive personalized training by a company-provided DSS. The DSS provides comprehensive education on Optune, including instruction on that patient’s individualized transducer array placement. Array mapping can be processed by Novocure internally or by clinicians who have leased NovoTAL™, Novocure’s proprietary treatment planning software. Maps used for guidance on array placement are generated from an MRI scan and are used by the team of physicians as a guide to general array placement (see Figure 2). 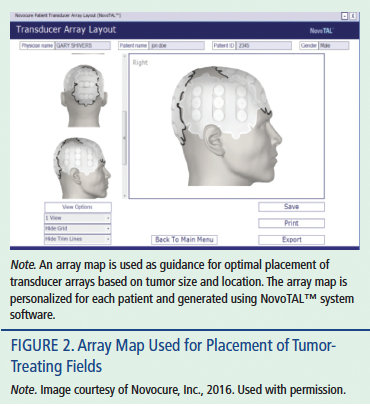
Available Support
In an effort to address any challenges related to TTFields therapy adherence, Novocure provides several resources for patients and their caregivers. As previously mentioned, the DSS team provides technical support to patients and meets with the patient on a monthly basis to download a compliance report directly from the device, which is also provided to the care team. This creates a platform to troubleshoot any technical or participant errors and creates an opportunity to reeducate patients and caregivers as needed. For example, patients with GBM often suffer from cognitive impairment and may forget to turn the device back on properly after a bathroom break and be unaware that treatment was never restarted. Based on the compliance report generated by the device, the DSS can identify this challenge and introduce practical solutions to increase adherence. Patients have access to a 24/7 technical hotline that provides remote instruction to address any alarms or issues of an unknown source. Although technical support is important for successful therapy adherence, patients must still be instructed to report any symptoms to their clinical team.
Support is also available from the Novocure company to assist with traveling considerations. Guidance documents and letters for air travel are available to inform patients of restrictions and allowances in an effort to promote safety and consistent compliance. Advance shipment of equipment to destinations is also available to lessen cumbersome luggage coordination.
Insurance Coverage
As with all medical therapies, insurance coverage will vary from patient to patient. As a durable medical equipment provider, Novocure can advocate on behalf of the patient to their insurance company. Novocure’s nCompassTM patient support program provides patients and caregivers with all aspects of incorporating the second-generation Optune system into treatment of GBM.
Practical Concerns for Managing Arrays and Equipment
Patients and their caregivers should be informed of several guidelines and recommendations when using Optune during activities of daily living.
Transducer arrays should be changed regularly, at least every four days. Any time the transducer arrays become wet or loosen, they should be changed. Showering or bathing with a shower cap is necessary to prevent the transducer arrays from getting wet. The device should remain outside the bathroom when bathing and should not be exposed to water. Patients may regard the array change as an opportunity to swim or take a temporary break from the arrays and device. In rainy weather, a hat or umbrella should be used to prevent the arrays from becoming damp.
Some warming of the scalp by device activity is expected. Overheating, which can result in device alarms, is avoided by use of breathable or light wigs, hats, or head coverings. Pillows that allow maximum circulation may be helpful if overheating is causing frequent overnight alarming.
To remove arrays, apply baby oil to the scalp, and slowly and gently peel back the arrays from the skin. Pulling the skin can contribute to skin breakdown and irritation.
Adverse Events
TTFields therapy provides a viable treatment option, particularly for those patients who cannot tolerate chemotherapy because of bone marrow suppression (Stupp et al., 2012, 2015). The most common (10% or greater) adverse events reported when using Optune alone were scalp irritation from device usage and headache. Nausea, vomiting, and seizure were infrequent side effects. Because of the heat generated from the arrays, special attention must be paid to cranial skin management (Stupp et al., 2012). Therefore, adequate skin preparation is crucial for good array adherence. Attention to good scalp care and array placement is necessary for maintaining skin integrity. Patients and caregivers should be instructed to evaluate the skin and scalp with every array change. Complete hair removal is required for optimal adhesion, and the scalp should be shaved every time the arrays are changed. The device generates low-frequency heat, which does not burn intercranial or intracranial tissue (Gabriel, Lau, & Gabriel, 1996). However, repeated exposure mixed with natural oils and perspiration can generate dermatologic adverse events; the most prevalent include allergic or irritant dermatitis (see Figure 3), folliculitis, erosions, secondary cutaneous infections, and ulcerations (Lacouture et al., 2014). 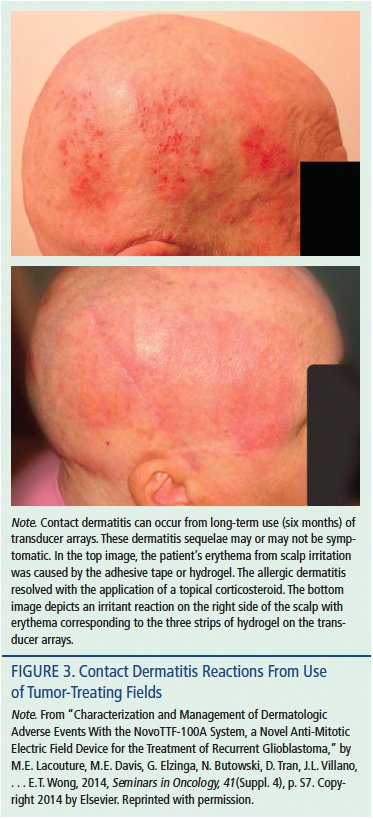
Management of adverse effects can be prevented or minimized by proactive education and using supporting material specifically prepared for patients and their families (see Figure 4). Figure 5 highlights a comprehensive list of many of the available measures to prevent dermatologic adverse events (Novocure, 2015). 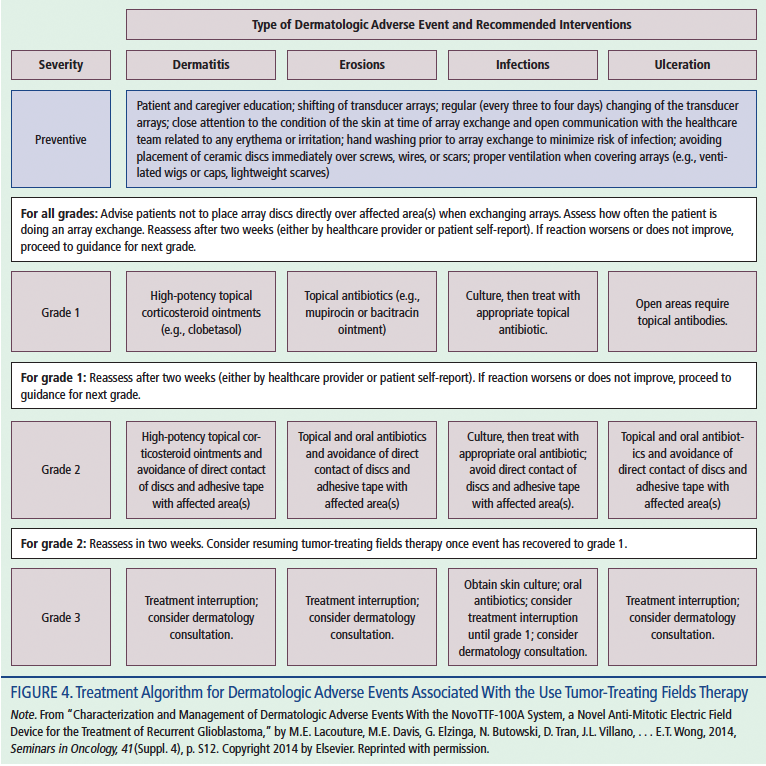
Guidance for management of adverse events is outlined in printed material that Novocure provides to treating centers. Skin irritation or rash may appear as redness under the transducer arrays. Some proactive, practical suggestions for clinicians and practitioners are listed. High-potency topical corticosteroids, such as clobetasol propionate or hydrocortisone, can be recommended for mild to moderate dermatitis. Ointments are preferable to creams because the compounds are more suited for skin absorption. The patient or caregiver should be instructed to apply the ointment to the dry scalp after array removal and showering or cleaning, letting it remain on the scalp for a minimum of 15–20 minutes. Before a new set of arrays is affixed to the scalp, the ointment should be wiped off and 70% isopropyl alcohol applied and allowed to completely dry. If not treated, skin irritation may become more serious, leading to skin breakdown, infections, and blisters. Infections should be addressed with topical or oral antibiotics; typical medications include topical bacitracin or oral doxycycline. Affected areas may be protected with nonadherent dressing, such as Telfa™, to protect against direct disc contact. The discs must make direct contact with the skin for the device to generate the fields. The device will emit an alarm if contact is lost. Severe erosions or ulcerations warrant complete treatment and array contact interruption until symptoms are fully resolved.
[[{"type":"media","view_mode":"media_original","fid":"26231","attributes":{"alt":"","class":"media-image","height":"369","typeof":"foaf:Image","width":"370"}}]]
Conclusion
New developments in oncology continue to transform therapeutic approaches for patients with cancer. TTFields therapy is one such therapeutic option that offers an innovative and alternative addition to traditional standard-of-care therapy for patients with GBM. Oncology nurses play a key role in Optune therapy for patients with GBM; they facilitate compliance and support patients’ quest for maintaining quality of life. Many resources are available to educate patients and clinicians on TTFields therapy, including adverse event management, maintaining desired activity level, and troubleshooting technical issues. Patients who are willing and have an active support system are more likely to have a successful integration of TTFields therapy into daily living. For appropriate patients, TTFields therapy can work in tandem with available standard-of-care treatments. Optune provides a therapy that empowers patients with GBM to proactively fight the progression of their disease.
[[{"type":"media","view_mode":"media_original","fid":"26236","attributes":{"alt":"","class":"media-image","height":"234","typeof":"foaf:Image","width":"375"}}]]
References
Chaudhry, A., Benson, L., Varshaver, M., Farber, O., Weinberg, U., Kirson, E., & Palti, Y. (2015). NovoTTF™-100A System (Tumor Treating Fields) transducer array layout planning for glioblastoma: A NovoTAL™ system user study. World Journal of Surgical Oncology, 13, 316. doi:10.1186/s12957-015-0722-3
Gabriel, S., Lau, R.W., & Gabriel, C. (1996). The dielectric properties of biological tissues: III. Parametric models for the dielectric spectrum of tissues. Physics in Medicine and Biology, 41, 2271–2293.
Gera, N., Yang, A., Holtzman, T.S., Lee, S.X., Wong, E.T., & Swanson, K.D. (2015). Tumor treating fields perturb the localization of septins and cause aberrant mitotic exit. PLoS One, 10, e0125269.
Kirson, E.D., Schneiderman, R.S., Dbaly, V., Tovarys, F., Vymazal, J., Itzhaki, A., . . . Palti, Y. (2009). Chemotherapeutic treatment efficacy and sensitivity are increased by adjuvant alternating electric fields (TTFields). BMC Medical Physics, 9, 1. doi:10.1186/1756-6649-9-1
Lacouture, M.E., Davis, M.E., Elzinga, G., Butowski, N., Tran, D., Villano, J.L., . . . Wong, E.T. (2014). Characterization and management of dermatologic adverse events with the NovoTTF-100A System, a novel anti-mitotic electric field device for the treatment of recurrent glioblastoma. Seminars in Oncology, 41(Suppl. 4), S1–S14.
Lee, S.X., Wong, E.T., & Swanson, K.D. (2011). Mitotic interference of cancer cells during anaphase by electric field from NovoTTF-100A. Neuro-Oncology, 13, iii13–iii14.
Mrugala, M.M., Engelhard, H.H., Tran, D.D., Kew, Y., Cavaliere, R., Villano, J.L., . . . Butowski, N. (2014). Clinical practice experience with NovoTTF-100A™ system for glioblastoma: The Patient Registry Dataset (PRiDe). Seminars in Oncology, 41(Suppl. 6), S4-S13.
Optune®. (2016). The Optune® system. Retrieved from http://www.optune.com/HCP/therapy/system.aspx
Novocure. (2015). Management guidelines of dermatologic adverse events [Brochure]. New York, NY: Author.
Rulseh, A.M., Keller, J., Klener, J., Sroubek, J, Dbaly, V., Syrucek, M., . . . Vymazal, J. (2012). Long-term survival of patients suffering from glioblastoma multiforme treated with tumor-treating fields. World Journal of Surgical Oncology, 10, 220.
Stupp, R., Tallibert, S., Kanner, A.A., Kesari, S., Steinberg, D.M., Toms, S.A., . . . Ram, Z. (2015). Maintenance therapy with tumor-treating fields plus temozolomide vs temozolomide alone for glioblastoma: A randomized clinical trial. JAMA, 314, 2535–2543.
Stupp, R., Wong, E.T., Kanner, A.A., Steinberg, D., Engelhard, H., Heidecke, V., . . . Gutin, P.H. (2012). NovoTTF-100A versus physician’s choice chemotherapy in recurrent glioblastoma: A randomized phase III trial of a novel treatment modality. European Journal of Cancer, 48, 2192–2202.
Wong, E.T., Lok, E., Gautam S., & Swanson, K.D. (2015). Dexamethasone exerts profound immunologic interference on treatment efficacy for recurrent glioblastoma. British Journal of Cancer, 113, 232–241.
About the Author(s)
Janlyn Murphy, BS, is a neuro-oncology clinical research coordinator, Mary Ellen Bowers, RN, MS, is a research RN, and Loretta Barron, NP, is a nurse practitioner, all in the Brain Tumor Program and Neuro-Oncology Unit at the Beth Israel Deaconess Medical Center in Boston, MA. The authors take full responsibility for the content of the article. Murphy has previously consulted for Novocure, Inc. Editorial support was provided by Stephen Swyberius, BA, copy supervisor at PharmaHealthLabs, through support from Novocure, Inc. The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. No financial relationships relevant to the content of this article have been disclosed by the independent peer reviewers or editorial staff. Mention of specific products and opinions related to those products do not indicate or imply endorsement by the Clinical Journal of Oncology Nursing or the Oncology Nursing Society. Murphy can be reached at jmurphy7@bidmc.harvard.edu, with copy to editor at CJONEditor@ons.org. (Submitted May 2016. Revision submitted July 2016. Accepted for publication July 21, 2016.)


