Lifestyle Counseling Practices of Oncology Nurses in the United States and Canada
Background: Oncology nurses are well poised to provide lifestyle behavior counseling to cancer survivors. However, very little is known about the current lifestyle behavior counseling practices of oncology nurses.
Objectives: The primary purpose of this study was to examine lifestyle behavior counseling practices of oncology nurses. The secondary purpose was to examine differences in lifestyle behavior counseling based on nurses’ health behaviors, additional training received, and country of residence.
Methods: Oncology nurses (N = 314) were primarily recruited through emails from oncology nursing email lists. Participants completed an online survey.
Findings: Overall, oncology nurses reported providing lifestyle counseling to most cancer survivors when appropriate. The majority of oncology nurses said they were receptive to receiving additional training about lifestyle counseling. Participants who had received additional training and who lived in the United States were more likely to provide counseling to cancer survivors. Concerning their own health behaviors, no meaningful differences were found regarding lifestyle behavior counseling practices, which contrasts with findings from previous research. Strengthening oncology nurses’ lifestyle behavior counseling knowledge and skills may offer opportunities to enhance survivors’ optimal health and quality of life and to reduce their risk of recurrence.
Jump to a section
Recommendations for optimal health during cancer survivorship include the practice of health-promoting lifestyle behaviors, such as engaging in regular physical activity, eating a healthy diet, and avoiding tobacco (Howell et al., 2011). However, population-based surveys suggest that cancer survivor populations are less likely than noncancer populations to practice lifestyle behaviors that may promote optimal health and well-being (Coups & Ostroff, 2005; Milliron, Vitolins, & Tooze, 2013; Pacheco-Figueiredo, Antunes, Bento, & Lunet, 2011). Data from the 2009 National Health Interview Survey suggested that 18% of cancer survivors were current smokers and 44% were physically inactive (Harding, 2012). Similarly, according to data from the 2003–2006 National Health and Nutrition Examination Survey, more than 90% of cancer survivors did not meet National Cancer Institute recommendations for fruit and vegetable intake (Milliron et al., 2013). The practice of unhealthy lifestyle behaviors can be detrimental for any individual, given the established links with increased risk of chronic disease and premature mortality (Eyre et al., 2004). After cancer diagnosis, this practice can also negatively affect survival times, increase the risk of recurrence, and contribute to lower quality of life (Cowens-Alvarado et al., 2013). However, mounting evidence points toward the beneficial role that healthy lifestyle behaviors play in survivors’ quality of life and disease-free survival (Campbell, Stevinson, & Crank, 2012; Courneya & Friedenreich, 2010; Davies, Batehup, & Thomas, 2011; Florou, Gkiozos, Tsagouli, Souliotis, & Syrigos, 2014; Ligibel, 2012; Loprinzi & Lee, 2014).
Although making healthier changes in lifestyle behaviors can be difficult for all populations, it becomes an even greater challenge for cancer survivors who face additional hurdles because of the stresses of cancer and its treatments (e.g., psychological distress, coping with side effects) (Cooley, Lundin, & Murray, 2009; Husebø, Karlsen, Allan, Søreide, & Bru, 2015; Reilley, Jacobs, Vaughn, & Palmer, 2014). Given their increasingly prominent role as a source of patient education and cancer expertise, oncology nurses are an important support resource for lifestyle behavior changes (Gosselin-Acomb, 2006). In addition, oncology nurses have frequent contact with cancer survivors throughout the cancer trajectory and are generally respected as having expertise related to health promotion. Consequently, oncology nurses may be well positioned to provide ongoing education and support centered on positive lifestyle behavior change for cancer survivors.
Relatively little is known about current lifestyle behavior counseling practices of oncology nurses. Having more information about these practices may be valuable for designing future lifestyle behavior interventions for cancer survivors. Only a paucity of surveys to date have assessed specific types of lifestyle behavior counseling practices among oncology care providers, such as tobacco cessation (Sarna et al., 2000), physical activity counseling (Karvinen, DuBose, Carney, & Allison, 2010; Karvinen, McGourty, Parent, & Walker, 2012), and weight loss (Anderson, Caswell, Wells, & Steele, 2013; Jernigan, Tergas, Satin, & Fader, 2013). Of these studies, few have focused specifically on oncology nurses, and some were limited to clinicians who specialize in caring for people with specific types of cancer.
The primary purpose of the current study was to explore oncology nurses’ lifestyle behavior counseling practices and beliefs. The secondary purpose was to assess if oncology nurses’ lifestyle behaviors, previous training in lifestyle behavior counseling, and geographic region have an effect on oncology nurses’ lifestyle behavior counseling practices and beliefs. Based on previous surveys by Karvinen et al. (2010, 2012) concerning physical activity counseling practices of oncology nurses, the current authors hypothesized in this study that participants would report providing lifestyle behavior counseling to the majority of patients. The current authors also expected that participants who practiced the healthiest lifestyle behaviors, as well as those who had received training in lifestyle behavior counseling, would provide lifestyle behavior counseling to a higher percentage of patients compared to those practicing unhealthier lifestyle behaviors and who had not received training in these practices. In addition, the current authors also hypothesized that general differences would exist in lifestyle behavior counseling practices between American and Canadian nurses given differences in healthcare systems (Buhr, 2013).
Methods
Study approval was obtained from the Nipissing University Research Ethics Board, and informed consent was waived. Participants in the study were required to be oncology nurses residing in the United States or Canada and currently seeing patients in a clinical capacity. Potential participants were recruited primarily from email lists of members of the Canadian Association of Nurses in Oncology (CANO-ACIO) and the Oncology Nursing Society (ONS). Emails were sent to the entire email list of CANO-ACIO (about 1,000) and to 4,000 randomly selected email addresses from the ONS membership list. The recruitment email included a brief description of the study and a link to the anonymous Internet-based survey. An opt-out option was included in the emails. Participants were offered the opportunity to enter into a drawing for a gift card. Two nurses responded by email to the current authors indicating that they no longer saw patients in a clinical capacity and were ineligible. A total of 314 completed surveys were received.
Instrument
Lifestyle behavior counseling practice: Lifestyle behavior counseling practice was assessed with two questions that began with the following stem: “To what percentage of patients with cancer on active treatment/post-treatment do you provide guidance or advice to concerning . . . (when appropriate)?” The questions ended with four options: “physical activity,” “diet,” “tobacco,” and “weight loss.” A third variable that combined active treatment and post-treatment by finding the average of the two values was also created. The items were based on those used in previous surveys developed by the lead author that assessed physical activity promotion among oncology nurses and oncologists (Karvinen et al., 2010, 2012).
Other items related to lifestyle behavior counseling: Seven additional items assessed variables related to lifestyle behavior counseling practices and training and were created by the current authors. Items were evaluated individually by the authors for face validity. Three items queried training, two items asked about time spent engaging in discussions concerning lifestyle behaviors, and two inquired about who should be providing lifestyle behavior counseling.
Fruit and vegetable intake: The 5 A Day fruit and vegetable screener, which consists of 16 items that measure fruit and vegetable consumption, was used to measure fruit and vegetable intake (Thompson et al., 2000). The screener has performed similarly to a food frequency questionnaire for relative risk estimates. When compared to actual intake, the median intake from the screener estimated true intake by 88% (Thompson et al., 2000).
Tobacco use: A single item that queried the number of tobacco products used in a typical day measured tobacco use. For the purposes of the study, tobacco use was quantified by a dichotomous measure (tobacco user versus nontobacco user). The criterion for “tobacco user” was the use of tobacco at least once per day in the past week.
Physical activity: A modified version of the Godin Leisure Time Physical Activity Questionnaire assessed physical activity (Godin & Shephard, 1985). Participants reported the number of physical activity sessions they completed in a typical week during the past month in addition to the average number of minutes per session. Three separate variables were created that summed weekly physical activity minutes based on intensity (i.e., light, moderate, or vigorous). From this data, physical activity variables were created based on global public health guidelines for aerobic exercise that recommend adults accumulate 150 minutes per week of moderate- to vigorous-intensity physical activity or 75 minutes of vigorous-intensity activity per week (World Health Organization, 2010). The first variable was average weekly moderate to vigorous physical activity (MVPA), calculated by adding weekly minutes of moderate and vigorous intensity physical activity together. The second was a dichotomous variable that categorized participants as meeting or not meeting global public health recommendations for physical activity (i.e., accumulating 150 minutes or more of weekly MVPA and/or 75 minutes of vigorous-intensity physical activity per week or not).
Alcohol consumption: One item assessed the number of alcoholic beverages consumed in a typical week and was based on the alcohol consumption module of the Behavioral Risk Factor Surveillance System survey (Centers for Disease Control and Prevention, 2011).
Demographic and professional information: Items that queried age, gender, ethnicity, country of residency, area of specialization, and years practicing nursing assessed demographic and professional information.
Statistical Analyses
SPSS®, version 22.0, was used for statistical analyses. A significant p value was set at 0.05. Descriptive statistics—including means, standard deviations, frequencies, and percentages—were used to analyze all data. Associations between oncology nurses’ lifestyle behavior counseling practices (combined on active- and post-treatment variable) and the corresponding oncology nurses’ lifestyle behaviors were analyzed using Pearson correlation coefficients (i.e., physical activity counseling and MVPA, diet counseling and fruit and vegetable intake, tobacco cessation counseling and smoking, weight loss counseling and MVPA and fruit and vegetable intake). Differences in lifestyle behavior counseling practices were analyzed based on (a) training in lifestyle behavior counseling and (b) country of residence using independent samples t tests.
Results
Descriptive statistics of demographic and professional information indicated that the mean age of participants was 47.7 years (SD = 10.8). In addition, the majority of participants were female (98%), most were Caucasian (90%), the majority lived in the United States (64%), and the most common specialization was chemotherapy (72%) (see Table 1). Detailed descriptive data of lifestyle behavior counseling variables are displayed in Tables 2 and 3. In brief, participants reported providing physical activity, diet, tobacco cessation, and weight loss guidance to about 75%, 78%, 61%, and 48% of patients, respectively, who could potentially make positive changes. Participants reported being “somewhat trained” to “well trained” in lifestyle behavior counseling. The majority indicated “yes” (66%–77%) or “maybe” (10%–13%) when asked if they would be interested in receiving training in lifestyle behavior counseling. Participants (62%–77%) also indicated that they felt oncology nurses should be responsible for providing lifestyle behavior counseling to patients. Bivariate correlations between participants’ lifestyle behaviors (MVPA, fruit and vegetable intake, and smoking) and lifestyle behavior counseling (physical activity, diet, tobacco, and weight loss) did not yield significant correlations (see Table 4). 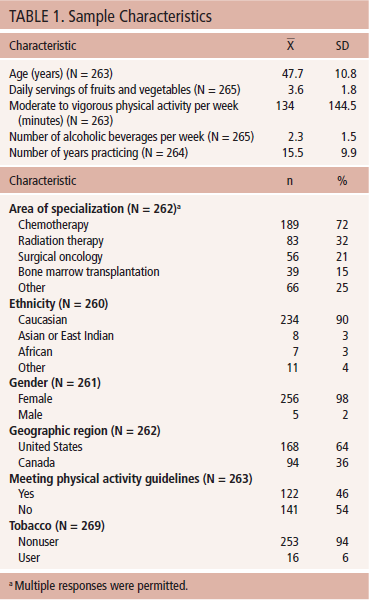
Significant differences emerged when comparisons were made in lifestyle behavior counseling practices between participants who had received training in a specific lifestyle behavior and those who had not. Participants who had received training on how to provide physical activity counseling were more likely to provide physical activity counseling to a greater percentage of patients on average (mean = 79%, SD = 22.3) compared to those who had not received training (mean = 70.7%, SD = 24.7; t[256] = 2.85, p = 0.005). A significantly higher percentage of participants who had received training in tobacco cessation and weight loss counseling provided the corresponding counseling to patients compared to those who had not received training (tobacco cessation: mean = 68.6%, SD = 34 versus mean = 55.1, SD = 33.1, t[255] = 3.24, p = 0.001; weight loss counseling: (mean = 58.4%, SD = 33.7 versus mean = 44.5, SD = 28.8, t[231] = 3.31, p = 0.001) compared to those who had not. No significant differences were observed in diet counseling practices between participants who had received training in diet counseling and those who had not (p > 0.05). 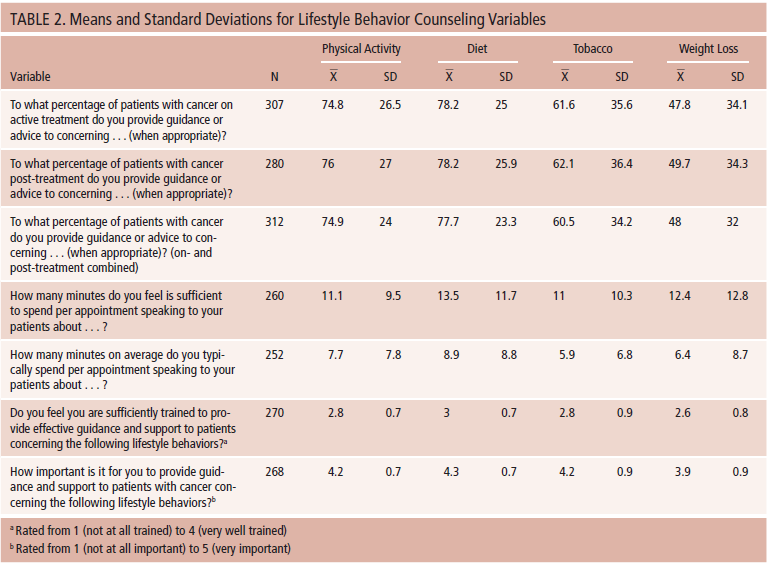
When comparing participants by country, participants from the United States were more likely to provide tobacco cessation counseling compared to those from Canada (mean = 66.7%, SD = 34.2 versus mean = 53.5, SD = 32.2; t[254] = 3, p = 0.003). This was also true for weight loss counseling (mean = 51.6%, SD = 32 versus mean = 42.5, SD = 30.3; t[231] = 2.11, p = 0.036). No significant differences were found between American and Canadian participants in physical activity or diet counseling practices (p > 0.05). 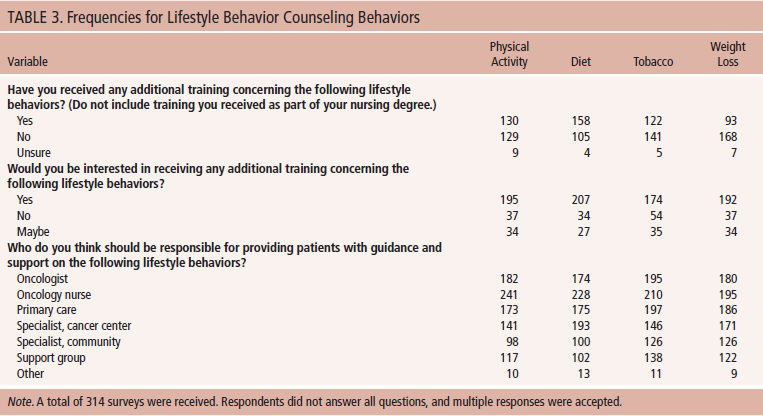
Discussion
This study found partial support for the current authors’ hypotheses and is generally consistent with previous research in lifestyle behavior counseling in oncology care settings (Jernigan et al., 2013; Karvinen et al., 2010, 2012; Sarna et al., 2000). Overall, the findings suggest that oncology nurses are willing to provide lifestyle behavior guidance and support to patients.
Consistent with the current authors’ hypotheses, oncology nurses reported providing lifestyle behavior counseling and support to the majority of their patients, particularly in terms of physical activity and diet counseling. In the study sample, the percentage of patients provided with physical activity guidance by oncology nurses was much higher than in a previous similar survey of oncology nurses by Karvinen et al. (2012) (75% versus 66%). Similarly, a past survey indicated that counseling on tobacco cessation among oncology nurses was fairly low, with only 36% of oncology nurses regularly providing counseling to patients (Sarna et al., 2000), compared to the findings in this study in which nurses reported counseling about 60% of appropriate patients (i.e., tobacco users). A more recent survey by Jernigan et al. (2013) indicated that of gynecologic oncology providers, including nurses, 54% regularly inquired about patients’ healthy eating habits, 62% about physical activity, and 29% about weight loss. The seemingly higher rates of lifestyle behavior counseling in the current study may be because of differences in the structure of the items in the surveys and because a sharp increase has occurred in the availability of information on the importance of practicing healthy lifestyle behaviors in cancer survivorship (Alfano, Molfino, & Muscaritoli, 2013). 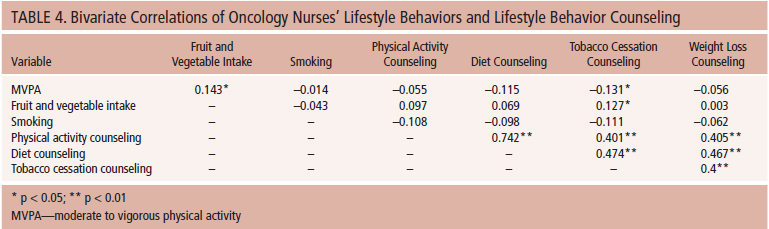
Oncology nurses in the current study were generally positive about providing lifestyle behavior counseling, even though they felt only “somewhat trained” to “well-trained” in doing so and were largely interested in receiving additional training. These findings are similar to past research that suggests that oncology nurses may not feel sufficiently trained to provide lifestyle behavior counseling to patients. For example, Sarna et al. (2000) indicated that three of the top barriers for providing tobacco cessation counseling included “lack of skill,” “lack of knowledge about how to help patients quit,” and “lack of knowledge, in general.” Similarly, Karvinen et al. (2012) found that “unsure what to recommend” and “unsure that physical activity is safe” were among the top barriers that oncology nurses reported as preventing them from providing physical activity counseling. However, the current survey and past research suggest that oncology nurses are interested in receiving additional training in lifestyle behavior change. In a survey of colorectal cancer clinicians, Anderson et al. (2013) found that 50% of respondents indicated that they would value additional training in weight management in patients with colorectal cancer. In an earlier survey, 92% of oncology nurses indicated they needed additional training in tobacco cessation counseling (Sarna et al., 2000). Oncology nurses appear to be eager to receive, and may benefit from, additional training concerning lifestyle behavior counseling.
No meaningful significant differences were observed regarding lifestyle behavior counseling practices based on participants’ physical activity level, fruit and vegetable intake, and smoking status. This finding is contrary to findings from previous research that revealed that physically active clinicians were more likely to provide physical activity counseling to patients (Karvinen et al., 2010, 2012) and from a survey that found that overweight or obese cancer care clinicians were less likely to place importance on addressing weight and lifestyle modifications in patients (Jernigan et al., 2013). The discrepancy between findings from the current study and those of past research may be attributable to a ceiling effect from higher rates of lifestyle behavior counseling in the current study, making it more difficult to statistically detect differences.
As expected, oncology nurses who had received additional training in a type of lifestyle behavior were more likely to provide counseling in that particular lifestyle behavior to patients. Past research with nurses has indicated that their having received additional training in tobacco control (Sheffer, Barone, & Anders, 2011) and obesity management (Huber et al., 2011) was associated with better lifestyle behavior counseling practices. These findings highlight the need for additional training opportunities for oncology nurses in lifestyle behavior counseling. For example, a number of documents exist that outline best practice guidelines by the American Cancer Society for nutrition, physical activity, and weight management for cancer survivors (Rock et al., 2012), as well as continuing education articles on behavior change strategies (Levensky, Forcehimes, O’Donohue, & Beitz, 2007).
The current authors identified some differences in lifestyle behavior counseling practices between American and Canadian participants. Specifically, the current authors found that oncology nurses from the United States provided tobacco cessation and weight loss guidance to a greater percentage of patients compared to Canadian oncology nurses. However, no differences were observed in physical activity or diet guidance. Differences in work environment may lead to greater rates of certain types of lifestyle behavior counseling in the United States compared to Canada. For example, past research determined that Canadian nurses, when compared to American nurses, reported higher workload, staffing inadequacy, and less autonomy in their work (Cameron, Armstrong-Stassen, Rajacich, & Freeman, 2010)—factors that may lead to less opportunity for providing lifestyle behavior counseling.
Limitations
The current study has a number of limitations that should be acknowledged. The response rate was fairly low (8%); however, poor response rates have been frequently observed in research surveying nurses, according to a systematic review by Van Geest and Johnson (2011). A low response rate may also have introduced bias with oncology nurses who value lifestyle behavior counseling self-selecting into the study, and/or those who do not believe lifestyle behavior counseling is within their scope of practice choosing not to participate. In addition, as with any self-report measures, participants likely overestimate socially acceptable behaviors, such as lifestyle behavior counseling practices. The lifestyle behavior counseling items also were created by the authors and have not been tested for validity and reliability beyond face validity. Because of the cross-sectional design of the study, interpretation of causal relationships between variables is not possible. 
Implications for Practice and Conclusion
Data from the current study were among the first to simultaneously explore several lifestyle behavior counseling practices of oncology nurses in the United States and Canada. Results suggest that although, on average, oncology nurses provide lifestyle behavior counseling to most of their patients, many patients still may not be receiving guidance and support. Overall, oncology nurses feel that they are responsible for doing so and that providing lifestyle behavior counseling to patients is important. Many believe they are only “somewhat trained” to provide lifestyle behavior counseling, and the majority indicate that they would like to receive additional training. Some differences in lifestyle behavior counseling practices were found based on previous training received and country of residence.
According to the current study, an important factor that influences lifestyle behavior counseling is having received additional training in the specific lifestyle behavior. As a result, oncology nurses may benefit from seeking further sources of training for the provision of lifestyle behavior counseling to patients. Oncology nursing organizations frequently offer courses and additional learning opportunities for oncology nurses that are centered on lifestyle behaviors. As the importance of lifestyle behavior change in cancer survivorship becomes increasingly apparent, oncology nurses may become integral in providing education and support for survivors to modify their lifestyle behaviors to achieve optimal health and quality of life, as well as reduce risk of recurrence. 
References
Alfano, C.M., Molfino, A., & Muscaritoli, M. (2013). Interventions to promote energy balance and cancer survivorship: Priorities for research and care. Cancer, 119, 2143–2150. doi:10.1002/cncr.28062
Anderson, A.S., Caswell, S., Wells, M., & Steele, R.J.C. (2013). Obesity and lifestyle advice in colorectal cancer survivors—How well are clinicians prepared? Colorectal Disease, 15, 949–957. doi:10.1111/codi.12203
Buhr, K. (2013). Access to medical care: How do women in Canada and the United States compare? Preventive Medicine, 56, 345–347. doi:10.1016/j.ypmed.2013.02.010
Cameron, S., Armstrong-Stassen, M., Rajacich, D., & Freeman, M. (2010). Working in Canada or the United States: Perceptions of Canadian nurses living in a border community. Nursing Leadership, 23, 30–45. doi:10.12927/cjnl.2010.21940
Campbell, A., Stevinson, C., & Crank, H. (2012). The BASES Expert Statement on exercise and cancer survivorship. Journal of Sports Sciences, 30, 949–952. doi:10.1080/02640414.2012.671953
Centers for Disease Control and Prevention. (2011). Behavioral risk factor surveillance system questionnaire. Retrieved from http://www.cdc.gov/brfss/questionnaires/pdf-ques/2011brfss.pdf
Cooley, M.E., Lundin, R., & Murray, L. (2009). Smoking cessation interventions in cancer care: Opportunities for oncology nurses and nurse scientists. Annual Review of Nursing Research, 27, 243–272. doi:10.1891/0739-6686.27.243
Coups, E.J., & Ostroff, J.S. (2005). A population-based estimate of the prevalence of behavioral risk factors among adult cancer survivors and noncancer controls. Preventive Medicine, 40, 702–711. doi:10.1016/j.ypmed.2004.09.011
Courneya, K.S., & Friedenreich, C.M. (2010). Physical activity and cancer: An introduction. Recent Results in Cancer Research, 186, 1–10. doi:10.1007/978-3-642-04231-7_1
Cowens-Alvarado, R., Sharpe, K., Pratt-Chapman, M., Willis, A., Gansler, T., Ganz, P.A., . . . Stein, K. (2013). Advancing survivorship care through the National Cancer Survivorship Resource Center: Developing American Cancer Society guidelines for primary care providers. CA: A Cancer Journal for Clinicians, 63, 147–150. doi:10.3322/caac.21183
Davies, N.J., Batehup, L., & Thomas, R. (2011). The role of diet and physical activity in breast, colorectal, and prostate cancer survivorship: A review of the literature. British Journal of Cancer, 105, S52–S73. doi:10.1038/bjc.2011.423
Eyre, H., Kahn, R., Robertson, R.M., Clark, N.G., Doyle, C., Hong, Y., . . . Thun, M.J. (2004). Preventing cancer, cardiovascular disease, and diabetes: A common agenda for the American Cancer Society, the American Diabetes Association, and the American Heart Association. CA: A Cancer Journal for Clinicians, 54, 190–207. doi:10.3322/canjclin.54.4.190
Florou, A.N., Gkiozos, I.C., Tsagouli, S.K., Souliotis, K.N., & Syrigos, K.N. (2014). Clinical significance of smoking cessation in subjects with cancer: A 30-year review. Respiratory Care, 59, 1924–1936. doi:10.4187/respcare.02559
Godin, G., & Shephard, R.J. (1985). A simple method to assess exercise behavior in the community. Canadian Journal of Applied Sport Sciences, 10, 141–146.
Gosselin-Acomb, T.K. (2006). Role of the radiation oncology nurse. Seminars in Oncology Nursing, 22, 198–202. doi:10.1016/j.soncn .2006.07.001
Harding, M. (2012). Health-promotion behaviors and psychological distress in cancer survivors. Oncology Nursing Forum, 39, E132–E140. doi:10.1188/12.ONF.E132-E140
Howell, D., Hack, T.F., Oliver, T.K., Chulak, T., Mayo, S., Aubin, M., . . . Sinclair, S. (2011). Survivorship services for adult cancer populations: A pan-Canadian guideline. Current Oncology, 18, e265–e281. doi:10.3747/co.v18i6.956
Huber, C.A., Mohler-Kuo, M., Zellweger, U., Zoller, M., Rosemann, T., & Senn, O. (2011). Obesity management and continuing medical education in primary care: Results of a Swiss survey. BMC Family Practice, 12, 140. doi:10.1186/1471-2296-12-140
Husebø, A.M., Karlsen, B., Allan, H., Søreide, J.A., & Bru, E. (2015). Factors perceived to influence exercise adherence in women with breast cancer participating in an exercise programme during adjuvant chemotherapy: A focus group study. Journal of Clinical Nursing, 24, 500–510. doi:10.1111/jocn.12633
Jernigan, A.M., Tergas, A.I., Satin, A.J., & Fader, A.N. (2013). Obesity management in gynecologic cancer survivors: Provider practices and attitudes. American Journal of Obstetrics and Gynecology, 208, 408.e1–408.e8. doi:10.1016/j.ajog.2013.02.002
Karvinen, K.H., DuBose, K.D., Carney, B., & Allison, R.R. (2010). Promotion of physical activity among oncologists in the United States. Journal of Supportive Oncology, 8, 35–41.
Karvinen, K.H., McGourty, S., Parent, T., & Walker, P.R. (2012). Physical activity promotion among oncology nurses. Cancer Nursing, 35, E41–E48. doi:10.1097/ncc.0b013e31822d9081
Levensky, E.R., Forcehimes, A., O’Donohue, W.T., & Beitz, K. (2007). Motivational interviewing: An evidence-based approach to counseling helps patients follow treatment recommendations. American Journal of Nursing, 107, 50–58.
Ligibel, J. (2012). Lifestyle factors in cancer survivorship. Journal of Clinical Oncology, 30, 3697–3704. doi:10.1200/JCO.2012.42.0638
Loprinzi, P.D., & Lee, H. (2014). Rationale for promoting physical activity among cancer survivors: Literature review and epidemiologic examination. Oncology Nursing Forum, 41, 117–125. doi:10.1188/14.ONF.117-125
Milliron, B.J., Vitolins, M.Z., & Tooze, J.A. (2013). Usual dietary intake among female breast cancer survivors is not significantly different from women with no cancer history: Results of the National Health and Nutrition Examination Survey, 2003–2006. Journal of the Academy of Nutrition and Dietetics, 114, 932–937. doi:10.1016/j.jand.2013.08.015
Pacheco-Figueiredo, L., Antunes, L., Bento, M.J., & Lunet, N. (2011). Health-related behaviours in the EpiPorto study: Cancer survivors versus participants with no cancer history. European Journal of Cancer Prevention, 20, 348–354. doi:10.1097/cej.0b013e328345f923
Reilley, M.J., Jacobs, L.A., Vaughn, D.J., & Palmer, S.C. (2014). Health behaviors among testicular cancer survivors. Journal of Community and Supportive Oncology, 12, 121–128.
Rock, C.L., Doyle, C., Demark-Wahnefried, W., Meyerhardt, J., Courneya, K.S., Schwartz, A.L., . . . Gansler, T. (2012). Nutrition and physical activity guidelines for cancer survivors. CA: A Cancer Journal for Clinicians, 62, 243–274. doi:10.3322/caac.21142
Sarna, L.P., Brown, J.K., Lillington, L., Rose, M., Wewers, M.E., & Brecht, M.L. (2000). Tobacco interventions by oncology nurses in clinical practice: Report from a national survey. Cancer, 89, 881–889.
Sheffer, C.E., Barone, C., & Anders, M.E. (2011). Training nurses in the treatment of tobacco use and dependence: Pre- and post-training results. Journal of Advanced Nursing, 67, 176–183. doi:10.1111/j.1365-2648.2010.05483.x
Thompson, F.E., Kipnis, V., Subar, A.F., Krebs-Smith, S.M., Kahle, L.L., Midthune, D., . . . Schatzkin, A. (2000). Evaluation of 2 brief instruments and a food-frequency questionnaire to estimate daily number of servings of fruit and vegetables. American Journal of Clinical Nutrition, 71, 1503–1510.
VanGeest, J., & Johnson, T.P. (2011). Surveying nurses: Identifying strategies to improve participation. Evaluation and the Health Professions, 34, 487–511. doi:10.1177/0163278711399572
World Health Organization. (2010). Global recommendations on physical activity for health. Retrieved from apps.who.int/iris/bitstream/10665/44399/1/9789241599979_eng.pdf
About the Author(s)
Kristina H. Karvinen, PhD, is an assistant professor and Brenda Bruner, PhD, is an associate professor, both in the School of Physical and Health Education at Nipissing University in North Bay, Ontario, and Tracy Truant, RN, MSN, is a doctoral candidate in the School of Nursing at the University of British Columbia in Vancouver, all in Canada. The authors take full responsibility for the content of the article. The authors did not receive honoraria for this work. The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. No financial relationships relevant to the content of this article have been disclosed by the authors, planners, independent peer reviewers, or editorial staff. Karvinen can be reached at kristinak@nipissingu.ca, with copy to editor at CJONEditor@ons.org. (Submitted January 2015. Revision submitted March 2015. Accepted for publication March 26, 2015.)