Integrating Geriatrics Into Oncology Ambulatory Care Clinics
Background: Geriatric oncology offers specialized care that incorporates comprehensive geriatric assessment (CGA) and multidisciplinary teams (MDTs) with oncology care. Geriatric syndromes, comorbidities, and caregiver concerns are relevant to the oncology assessment in older adult patients to make treatment decisions, which should be based not on age but on health and functional status, as well as on life expectancy. Developing a geriatric oncology ambulatory care clinic (GOACC) requires numerous resources and entails planning for longer patient encounter times, devising collaboration strategies with community care providers, and establishing dedicated time for team members.
Objectives: The purpose of this article is to provide information regarding the construction and sustainability of a GOACC.
Methods: A comprehensive review of literature published from 1991–2015 was conducted using the following key words: geriatric oncology, comprehensive geriatric assessment, supportive care, multidisciplinary, and elderly.
Findings: Oncology primary care nurses and advanced practice nurses have a large role in the development and maintenance of GOACCs. Managing comorbidities, identifying patients who likely would benefit from a CGA, providing caregiver support, conducting a CGA, and creating an MDT are core elements of developing a sustainable GOACC.
Jump to a section
More than 50% of new cancer diagnoses occur in people aged 65 years or older (National Cancer Institute [NCI], 2015). The median age of a cancer diagnosis in the United States is 65 years, and the median age of death associated with a malignancy is 72 years (NCI, 2015). Simply offering cancer care is insufficient to meet the healthcare needs of older adult patients and their families. Geriatric oncology offers cancer care and addresses relevant issues, such as preservation of independence, comorbid conditions, and caregiver support needs (Hurria, 2013; Tremblay, Charlebois, Terret, Joannette, & Latreille, 2012). Helping patients and families to understand that cancer treatment options are not exclusively based on chronological age but also on functional status and the existence of comorbidities (Hurria, 2013) can pave the way for more effective healthcare decisions.
Geriatric care extends beyond the general history and physical examination, assessing patients for the existence of geriatric syndromes (i.e., problems that have many causes, such as dementia and functional limitations), comorbidities, and psychosocial concerns (Hoffe & Balducci, 2012). For this reason, a geriatric oncology ambulatory care clinic (GOACC) is central to adequately treating older adults with cancer (Hurria et al., 2007; Marenco et al., 2008). Maintaining physical, mental, and social support status of older adult patients is critical to cancer treatment success (Balducci, 2005; Balducci, Colloca, Cesari, & Gambassi, 2010). In fact, geriatric oncology care may decrease three-year mortality in older adult patients because they are more likely to undergo surgery and receive chemotherapy (van de Water et al., 2014).
A GOACC often includes a comprehensive geriatric assessment (CGA) that can reveal various problems, such as cognitive, physical, and emotional changes (Klepin et al., 2011); postoperative complications (Fukuse, Satoda, Hijiya, & Fujinaga, 2005); toxicity to cancer chemotherapy treatment (Aaldriks et al., 2011; Freyer et al., 2005; Hurria & Lichtman, 2007); frailty (Kristjansson et al., 2010); and risk for falls (Overcash & Beckstead, 2008). A CGA is also helpful in identifying older adult patients with cancer who are most likely to benefit from aggressive chemotherapy (Tucci et al., 2009).
Geriatric oncology care is a layered process that requires expertise, considerable patience, multiple resources, and fastidious communication with general practitioners, other medical teams, and family members. Not all problems can be solved or even evaluated during one visit to the clinic. Patients and families must be committed to making multiple office visits, adhering to team recommendations, and consulting with specialists, such as physical therapists and mental and cognitive health professionals.
A formidable barrier to providing geriatric oncology care is that the development of a GOACC requires a multidisciplinary team (MDT) experienced in caring for older adults, as well as in executing intricate collaborations and clinic scheduling to support longer patient encounters (Sattar, Alibhai, Wildiers, & Puts, 2014). Despite some of the barriers, oncology clinics that specialize in the care of older adult patients are becoming more common, particularly at large medical centers, such as the H. Lee Moffitt Cancer Center and Research Institute in Tampa, Florida, and the City of Hope National Medical Center in Duarte, California (McNeil, 2013). The intent of this article is to provide information for constructing an effective and sustainable GOACC. 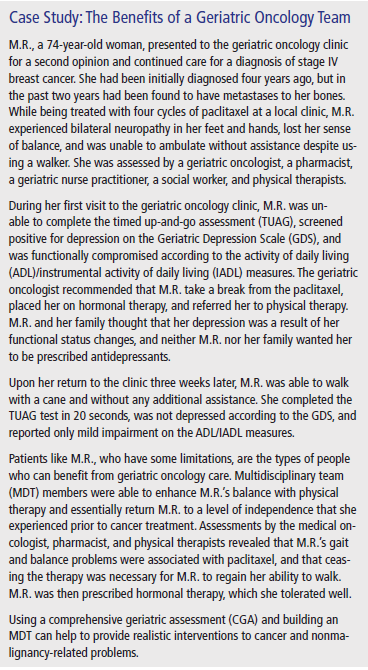
Navigating the Nonmalignant Conditions of Older Adults
Comorbid conditions or coexisting diagnoses are common with older age. The mean number of diagnoses for a person aged 70 years or older is 5.6 (Fried, Storer, King, & Lodder, 1991). Untreated comorbidities can increase the risk of chemotherapy toxicities (Chao et al., 2014), and addressing nonmalignant issues (e.g., cardiac problems) can help to lay a foundation for cancer treatment and reduce complications (e.g., congestive heart failure, cardiomyopathy) (Tsai, Pfeiffer, Warren, Wilson, & Landgren, 2015). Patients with moderate to severe comorbidities are likely to experience grade 3 or grade 4 nonhematologic toxicities from cancer treatment (Wildes et al., 2013). The likelihood of survival decreases with an increasing number of comorbidities (Koroukian, Bakaki, Schluchter, & Owusu, 2011).
After a cancer diagnosis, the focus of health care often becomes the malignancy, and many other comorbidities are put on hold until after cancer therapy. In reality, patients are more likely to succumb to cardiac problems than cancer-related problems (Centers for Disease Control and Prevention, 2015). If patients are receiving treatment from other providers for comorbidities, they should be encouraged to continue treatment and maintain appointments. In addition, medical records from the oncology visit concerning tumor and treatment type, as well as other relevant information, must be sent to patients’ primary care providers and other specialists. Adequate care of the older adult patient requires coordination among providers concerning medications, recommendations, and prescribed therapies to reduce duplicate billing, issues related to polypharmacy (excessive medications), and other problems associated with many prescribers (Holmes & Albrand, 2013).
For comorbidities discovered during oncology care, referrals to disease-specific services are necessary. Older adult women who develop comorbidities following a diagnosis of breast cancer have a higher all-cause mortality rate (Jordan et al., 2014). When considering the development of a GOACC, making connections with physicians who are willing to accept patients and work together to provide comprehensive care is vital. For academic medical centers, these connections may not be difficult to make, but for community clinics, establishing such relationships with referring physicians may be more difficult. Proactively seeking referral sources ensures that various practices are accepting new patients and are willing to work with cancer care providers.
Caregiver Support
About 29% of the adult population in the United States provides care to someone who is ill, disabled, or aged (Family Caregiver Alliance, 2012). However, caregiver and social support limitations are often primary concerns for health professionals when caring for older adults. About 11 million noninstitutionalized older adults live alone in the United States, with most being women living in poverty (Administration on Aging, 2011; U.S. Department of Health and Human Services, 2014). For many community-dwelling (i.e., not living in assisted living or another facility) older adults diagnosed with cancer, living alone is a disadvantage, particularly regarding communicating with healthcare professionals and traveling to medical appointments (Goodwin, Hunt, & Samet, 1991; Hanratty et al., 2013; Lynch, Marcone, & Kagan, 2007).
Care of patients and caregivers is important (Goldzweig et al., 2013). Some caregivers have the same or equivalent health limitations as patients (Meriggi et al., 2014; Sherman, 2008), and encouraging caregivers to maintain personal health is imperative so that they may preserve their caregiving role (Sherman, 2008). Because of responsibilities associated with patients and their illness, caregivers may not be as diligent with their own medical appointments. In addition, caregivers who experience moderate levels of strain have an enhanced risk of mortality during a four-year period (Schulz & Beach, 1999). Emotional health is also important to reduce strain and depression for caregivers. Caregivers report a high degree of burden, particularly when they are employed outside of the home and are caring for someone who is functionally dependent (Hsu et al., 2014). The MDT must encourage caregivers to seek support and maintain physical, emotional, and functional health. Support can be given to caregivers by acknowledging their challenges, providing education concerning the disease process and symptom management, and reducing symptom burden in patients (Hazelwood, Koeck, Wallner, Anderson, & Mayer, 2012).
Conducting a Comprehensive Geriatric Assessment in Ambulatory Care
A CGA is a global evaluation that addresses issues often not included in patients’ general history and physical examination, and is recommended by the International Society of Geriatric Oncology in the care of older adult patients with cancer (Extermann et al., 2005). Geriatric considerations include physical reserve (i.e., the ability to endure a health insult and return to the same level of functioning as before a malignancy) (Balducci, 2013) and life expectancy (Hurria et al., 2014); both are central to cancer treatment discussions. Dementia and delirium, incontinence, depression, and functional status limitations are also assessed using a CGA. A CGA may affect cancer treatment decisions during the initial planning of cancer treatment and in subsequent follow-up visits (Horgan et al., 2012). In addition, a CGA can help to predict survival in patients with cancer (Klepin et al., 2013), as well as signs of toxicity if baseline assessments are conducted prior to beginning chemotherapy (Hamaker et al., 2014). CGAs have been performed as inpatient consultations (Morin et al., 2012) in academic medical centers (Liu & Extermann, 2012) and in community ambulatory care clinics (Williams et al., 2014).
However, not every older adult patient will benefit from a CGA. Older age, multiple medications, and comorbidities are features of patients who are more likely to benefit from a CGA than those who have higher overall levels of health and do not require medications (Stijnen et al., 2014). To target the older adults most likely to benefit from a CGA, several prescreening tools have been developed. Generally, the prescreening requires only a few minutes to conduct, and the scores can determine who is likely to benefit from a CGA. The abbreviated CGA regarding older adult patients with cancer was developed by determining the most predictive items on the activity of daily living (ADL)/instrumental activity of daily living (IADL) measures, on the Geriatric Depression Scale (GDS), and on the Mini-Mental State Examination (Overcash, Beckstead, Moody, Extermann, & Cobb, 2006). In addition, the G-8 is a prescreening tool largely based on the Mini-Nutritional Assessment and age, and it is widely used internationally (Bellera et al., 2012). These types of prescreening tools are developed with the ambulatory clinic in mind so patients who are in most need of a CGA can be targeted. Time-saving measures are important, and perhaps more clinics will be willing to conduct CGAs if they can be performed in a reasonable amount of time.
Some types of screening are self-report measures, and they include the ADL (Katz, Downs, Cash, & Grotz, 1970) and IADL (Lawton & Brody, 1969) measures. Other measures are performance- based, such as the timed up-and-go assessment (Podsiadlo & Richardson, 1991) and the hand-grip test (Giampaoli et al., 1999). One advantage of self-report measures is that they can be completed prior to the clinic visit or over the phone, as is the case with the GDS (Burke, Roccaforte, Wengel, Conley, & Potter, 1995). Performance measures tend to require little time to perform and render empirical data. Other self-report instruments screen for various issues, including sleep problems, anxiety, and caregiver distress. Limiting the number of instruments included in a CGA to three or four may be useful, particularly if the clinic is new and needs to refine some of its organizational processes. Some screening measures, particularly those with sensitive interview items, may require some practice before an effective technique for conducting them is acquired; however, the process is not complicated. Respondent burden should be considered because many patients who receive care at academic medical centers are approached to complete questionnaires; not exhausting patients and their families is important (Ulrich, Wallen, Feister, & Grady, 2005).
Creating a Multidisciplinary Team
Primary care nurses, nurse practitioners, and physicians can administer a CGA. Members of the MDT may administer discipline-specific screening tools, such as the Mini-Nutritional Assessment (Vellas et al., 2000) or the Beers Criteria for Potentially Inappropriate Medication Use in Older Adults (Beers, 1997); a physical therapist may conduct the Berg Balance Test (Berg, Wood-Dauphinee, Williams, & Maki, 1992). About 75% of patients require recommendations regarding their medications and request a pharmacist. Social workers provide assistance to about 50% of the older adult patients and their families seen in ambulatory oncology clinics (Chapman, Swartz, Schoppe, & Arenson, 2014). The more frail the older adult patient, the more likely a social worker will be required (Bouzereau et al., 2013). Dietitians are useful to an MDT in detecting actual and potential problems (Vandewoude, 2010) because malnutrition becomes more prevalent with aging (Hickson, 2006; Vandewoude, 2010); many patients and caregivers report the need for more information regarding nutrition (Pinto et al., 2014).
Assembling an MDT comprised of physicians, nurses, social workers, physical therapists, pharmacists, and dietitians can be difficult. Team development requires a great deal of negotiation with administration for allocation of resources and time. Clearly defining and reserving time each week for the geriatric clinic may avoid overburdening members of an MDT with geriatric patients with cancer in addition to their regular responsibilities. Each department must dedicate a percentage of its time to the geriatric team, and realistic discussions about the time and responsibilities required from each team member are important to create a foundation for the geriatric oncology clinic. One person should be designated as the clinic coordinator to direct the team members, compile CGA data, and facilitate team discussion concerning the interpretation of scores and the development of recommendations. The coordinator can be any of the team members but must be able to dedicate time to organizing the team, assembling patient data, and offering follow-up communication with patients and families, among many other responsibilities. The coordinator role often falls to the primary care nurse or a nurse practitioner, and protected time must be provided.
Patient navigators can help older adult patients and families with the coordination of oncology and other healthcare services, reducing the time required for resolution of the cancer diagnosis (Lee et al., 2013). Navigators can help to organize oncology and noncancer-related medical appointments and recommendations; issues with self–managing various medical specialist appointments and knowledge deficits associated with cancer diagnoses are barriers to care (Pieters, Heilemann, Grant, & Maly, 2011). Navigators also can help to guide older adult patients through the geriatric oncology medical process. In addition, the role of the navigator includes helping with Medicare and other insurance issues. Older adult patients with cancer often want prompt information about Medicare coverage and supplemental insurance (Pisu, Martin, Shewchuk, & Meneses, 2014).
Working as a team is not without challenges. Patience, acceptance of roles, clear leadership, and tolerance are essential elements of effective teams. The team should meet regularly to discuss patients and operational issues of the clinic. Developing and maintaining the cohesiveness of the team is ongoing and requires conflict resolution, trust, and respect among members (Mellor, Davis, & Capello, 1997). Effective teams are nurtured and educated about principles associated with team membership (Fulmer, Flaherty, & Hyer, 2003). When identifying team members, individuals who can work together and provide the necessary expertise to support the efforts of the geriatric oncology program should be selected.
Sustainable Geriatric Care
Numerous resources are required to manage complicated issues associated with cancer and its treatment. Older adults tend to have more costly diagnoses, and they make up a great deal of the healthcare costs in the United States (Stanton, 2006). However, the cost of MDTs may be small when compared to the potential benefits (Simcock & Heaford, 2012). Administrators and office managers must recognize that geriatric care may not be as profitable as other services that manage less complex cases. Understanding that fewer patients will be seen during a clinic day as compared to other disease-specific services, as well as that more professional full-time units will be required to administer the CGA, is essential to sustain a geriatric clinic. The median time to complete a CGA, excluding other tasks generally performed in the oncology clinic, is 19 minutes in academic medical centers and 22 minutes in community clinics (Williams et al., 2014). Adding about 25–30 minutes to an oncology ambulatory care visit can practically double the time that an examination room is needed for one patient. Creating an infrastructure that will support the additional time required to conduct the CGA is important. Allotting 90 minutes of clinic time for new patients and 30–45 minutes for established patients will produce a realistic clinic schedule and provide the time necessary to conduct the CGA and create recommendations.
Being visible as a geriatric oncology clinic or provider can increase awareness of the clinic and the types of patients who should be referred to it. Some services refer patients for a one-time evaluation, whereas others fully refer patients for ongoing care. Discussions with administration about how patients are to be referred to the geriatric oncology clinic can help with scheduling and evaluating the patients who are in need, as well as with promoting geriatrics in an oncology setting. Presentations at team meetings throughout the facility can help other professionals to understand the specialized care that is offered. Many healthcare professionals are unaware of the benefits of geriatrics, particularly in an oncology setting. Prominent positioning of CGA scores and recommendations in the medical record may be welcomed by other specialists in the cancer center. Documentation of the geriatric encounter is evidence that geriatric care differs from traditional oncology care. Working with those who are in charge of the medical record (electronic or hard copy) to ensure that the geriatric encounter is included in the health record and clearly labeled (e.g., “senior adult oncology clinic,” “geriatric oncology clinic”) provides more visibility.
Implications for Nursing
GOACCs are a good fit for nurses who like to provide education, offer support, and truly engage in clinical assessment in older adults. Geriatrics is focused on the evaluation of small or covert problems that, if treated early, may prevent decline in functional status or independence (Lichtman, Balducci, & Aapro, 2007). Oncology nurses have excellent assessment skills and can be trained to conduct components of a comprehensive CGA. Documentation of the results of a CGA, MDT recommendations, and communication with outside providers are tasks primarily performed by the primary care or advanced practice nurse. Another large and important responsibility of nurses is coordinating care and communicating with families.
Within the scope of practice for primary care and advanced practice nurses is providing input into the development and management of geriatric oncology clinics. Nurses must be included in the development of the infrastructure to create sustainable clinics that work to address the needs of older adult patients with cancer. If nurses are to coordinate the MDT, they must participate in administrative discussions concerning the allocation of resources, as well as provide perspectives about clinic staffing and scheduling.
Promoting the role of the geriatric oncology nurse to undergraduate and graduate nursing programs can inspire curriculum development and interest at colleges and universities. Undergraduate assessment courses should include content to prepare nurses to conduct CGAs, particularly in regard to history taking, interviewing skills, and physical assessment. Geriatric care does not always take place in a nursing or long-term care facility; it is also provided in emergency rooms, intensive care units, and cardiology and oncology settings. Nurses are vital to geriatric oncology, and their training must include an understanding that the typical patient with cancer is aged 65 years or older (NCI, 2015). ![]()
Conclusion
Being aware of the issues of aging and the complexities of cancer care provides a holistic perspective for caring for older adults with cancer. Trained nurses will recognize and manage symptoms related to cancer care and identify toxicities associated with cancer treatment that may vary with the age of the patient. Developing a GOACC is more complex than simply adding assessment tools to the oncology clinic visit. The clinic needs to be prepared to address the needs of older adult patients and must be willing to schedule longer appointments, provide more professional full-time units, and ensure access to referrals for specialty services. Sustainable geriatric care must be cultivated, supported, and appreciated. Combining the geriatric specialty with oncology may mean that many older adult patients will receive more comprehensive assessment, appropriate interventions and referrals, and better quality of care.
About the Author(s)
Janine Overcash, PhD, GNP-BC, is an associate clinical professor in the College of Nursing at Ohio State University in Columbus. The author takes full responsibility for the content of the article. The author did not receive honoraria for this work. The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. No financial relationships relevant to the content of this article have been disclosed by the author, planners, independent peer reviewers, or editorial staff. Overcash can be reached at overcash.1@osu.edu, with copy to editor at CJONEditor@ons.org. (Submitted July 2014. Revision submitted October 2014. Accepted for publication October 14, 2014.)
References
Aaldriks, A.A., Maartense, E., le Cessie, S., Giltay, E.J., Verlaan, H.A., van der Geest, L.G., . . . Nortier, J.W. (2011). Predictive value of geriatric assessment for patients older than 70 years, treated with chemotherapy. Critical Reviews in Oncology/Hematology, 79, 205–212. doi:10.1016/j.critrevonc.2010.05.009
Administration on Aging. (2011). A profile of older Americans: 2011. Retrieved from https://www.acl.gov/aging-and-disability-in-america/data-and-research/p…
Balducci, L. (2005). Cancer chemotherapy in elderly cancer patients. Journal of Oncology Management, 14, 35–38.
Balducci, L. (2013). Frailty: A common pathway in aging and cancer. Interdisciplinary Topics in Gerontology, 38, 61–72. doi:10.1159/000343586
Balducci, L., Colloca, G., Cesari, M., & Gambassi, G. (2010). Assessment and treatment of elderly patients with cancer. Surgical Oncology, 19, 117–123. doi:10.1016/j.suronc.2009.11.008
Beers, M.H. (1997). Explicit criteria for determining potentially inappropriate medication use by the elderly. An update. Archives of Internal Medicine, 157, 1531–1536. doi:10.1001/archinte .1997.00440350031003
Bellera, C.A., Rainfray, M., Mathoulin-Pélissier, S., Mertens, C., Delva, F., Fonck, M., & Soubeyran, P.L. (2012). Screening older cancer patients: First evaluation of the G-8 geriatric screening tool. Annals of Oncology, 23, 2166–2172. doi:10.1093/annonc/mdr587
Berg, K.O., Wood-Dauphinee, S.L., Williams, J.I., & Maki, B. (1992). Measuring balance in the elderly: Validation of an instrument. Canadian Journal of Public Health, 83(Suppl. 2), S7–S11.
Bouzereau, V., Le Caer, F., Guardiola, E., Scavennec, C., Barriere, J.R., Chaix, L., & Le Caer, H. (2013). Experience of multidisciplinary assessment of elderly patients with cancer in a French general hospital during 1 year: A new model care study. Journal of Geriatric Oncology, 4, 394–401. doi:10.1016/j.jgo.2013.04.006
Burke, W.J., Roccaforte, W.H., Wengel, S.P., Conley, D.M., & Potter, J.F. (1995). The reliability and validity of the Geriatric Depression Rating Scale administered by telephone. Journal of the American Geriatrics Society, 43, 674–679. doi:10.1111/j.1532-5415.1995 .tb07205.x
Centers for Disease Control and Prevention. (2015). Deaths and mortality. Retrieved from http://www.cdc.gov/nchs/fastats/deaths.htm
Chao, C., Page, J.H., Yang, S.J., Rodriguez, R., Huynh, J., & Chia, V.M. (2014). History of chronic comorbidity and risk of chemotherapy-induced febrile neutropenia in cancer patients not receiving G-CSF prophylaxis. Annals of Oncology, 25, 1821–1829. doi:10.1093/annonc/mdu203
Chapman, A.E., Swartz, K., Schoppe, J., & Arenson, C. (2014). Development of a comprehensive multidisciplinary geriatric oncology center, the Thomas Jefferson University Experience. Journal of Geriatric Oncology, 5, 164–170. doi:10.1016/j.jgo.2014.01.003
Extermann, M., Aapro, M., Bernabei, R., Cohen, H.J., Droz, J.P., Lichtman, S., . . . Topinkova, E. (2005). Use of comprehensive geriatric assessment in older cancer patients: Recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Critical Reviews in Oncology/Hematology, 55, 241–252. doi:10.1016/j.critrevonc.2005.06.003
Family Caregiver Alliance. (2012). Selected caregiver statistics. Retrieved from https://www.caregiver.org/selected-caregiver -statistics
Freyer, G., Geay, J.F., Touzet, S., Provencal, J., Weber, B., Jacquin, J.P., . . . Pujade-Lauraine, E. (2005). Comprehensive geriatric assessment predicts tolerance to chemotherapy and survival in elderly patients with advanced ovarian carcinoma: A GINECO study. Annals of Oncology, 16, 1795–1800. doi:10.1093/annonc/mdi368
Fried, L.P., Storer, D.J., King, D.E., & Lodder, F. (1991). Diagnosis of illness presentation in the elderly. Journal of the American Geriatrics Society, 39, 117–123. doi:10.1111/j.1532-5415.1991.tb01612.x
Fukuse, T., Satoda, N., Hijiya, K., & Fujinaga, T. (2005). Importance of a comprehensive geriatric assessment in prediction of complications following thoracic surgery in elderly patients. Chest, 127, 886–891. doi:10.1378/chest.127.3.886
Fulmer, T., Flaherty, E., & Hyer, K. (2003). The geriatric interdisciplinary team training (GITT) program. Gerontology and Geriatrics Education, 24, 3–12. doi:10.1300/j021v24n02_02
Giampaoli, S., Ferrucci, L., Cecchi, F., Lo Noce, C., Poce, A., Dima, F., . . . Menotti, A. (1999). Hand-grip strength predicts incident disability in non-disabled older men. Age and Ageing, 28, 283–288. doi:10.1093/ageing/28.3.283
Goldzweig, G., Merims, S., Ganon, R., Peretz, T., Altman, A., & Baider, L. (2013). Informal caregiving to older cancer patients: Preliminary research outcomes and implications. Annals of Oncology, 24, 2635–2640. doi:10.1093/annonc/mdt250
Goodwin, J.S., Hunt, W.C., & Samet, J.M. (1991). A population-based study of functional status and social support networks of elderly patients newly diagnosed with cancer. Archives of Internal Medicine, 151, 366–370. doi:10.1001/archinte.1991.00400020114022
Hamaker, M.E., Seynaeve, C., Wymenga, A.N., van Tinteren, H., Nortier, J.W., Maartense, E., . . . Smorenburg, C.H. (2014). Baseline comprehensive geriatric assessment is associated with toxicity and survival in elderly metastatic breast cancer patients receiving single-agent chemotherapy: Results from the OMEGA study of the Dutch breast cancer trialists’ group. Breast, 23, 81–87. doi:10.1016/j.breast.2013.11.004
Hanratty, B., Addington-Hall, J., Arthur, A., Cooper, L., Grande, G., Payne, S., & Seymour, J. (2013). What is different about living alone with cancer in older age? A qualitative study of experiences and preferences for care. BMC Family Practice, 14, 22. doi:10.1186/1471-2296-14-22
Hazelwood, D.M., Koeck, S., Wallner, M., Anderson, K.H., & Mayer, H. (2012). Patients with cancer and family caregivers: Management of symptoms caused by cancer or cancer therapy at home. HeilberufeScience, 3, 149–158. doi:10.1007/s16024-012 -0118-z
Hickson, M. (2006). Malnutrition and ageing. Postgraduate Medical Journal, 82, 2–8. doi:10.1136/pgmj.2005.037564
Hoffe, S., & Balducci, L. (2012). Cancer and age: General considerations. Clinics in Geriatric Medicine, 28, 1–18. doi:10.1016/j .cger.2011.09.001
Holmes, H.M., & Albrand, G. (2013). Organizing the geriatrician/ oncologist partnership: One size fits all? Practical solutions. Interdisciplinary Topics in Gerontology, 38, 132–138. doi:10.1159/ 000343615
Horgan, A.M., Leighl, N.B., Coate, L., Liu, G., Palepu, P., Knox, J.J., . . . Alibhai, S.M. (2012). Impact and feasibility of a comprehensive geriatric assessment in the oncology setting: A pilot study. American Journal of Clinical Oncology, 35, 322–328. doi:10.1097/COC.0b013e318210f9ce
Hsu, T., Loscalzo, M., Ramani, R., Forman, S., Popplewell, L., Clark, K., . . . Hurria, A. (2014). Factors associated with high burden in caregivers of older adults with cancer. Cancer, 120, 2927–2935. doi:10.1002/cncr.28765
Hurria, A. (2013). Management of elderly patients with cancer. Journal of the National Comprehensive Cancer Network, 11(Suppl. 5), 698–701.
Hurria, A., & Lichtman, S.M. (2007). Pharmacokinetics of chemotherapy in the older patient. Cancer Control, 14, 32–43.
Hurria, A., Lichtman, S.M., Gardes, J., Li, D., Limaye, S., Patil, S., . . . Kelly, E. (2007). Identifying vulnerable older adults with cancer: Integrating geriatric assessment into oncology practice. Journal of the American Geriatrics Society, 55, 1604–1608. doi:10.1111/j.1532-5415.2007.01367.x
Hurria, A., Wildes, T., Blair, S.L., Browner, I.S., Cohen, H.J., Deshazo, M., . . . Sundar, H. (2014). Senior adult oncology, version 2.2014: Clinical practice guidelines in oncology. Journal of the National Comprehensive Cancer Network, 12, 82–126.
Jordan, J.H., Thwin, S.S., Lash, T.L., Buist, D.S., Field, T.S., Haque, R., . . . Geiger, A.M. (2014). Incident comorbidities and all-cause mortality among 5-year survivors of Stage I and II breast cancer diagnosed at age 65 or older: A prospective-matched cohort study. Breast Cancer Research and Treatment, 146, 401–409. doi:10.1007/s10549-014-3021-8
Katz, S., Downs, T.D., Cash, H.R., & Grotz, R.C. (1970). Progress in development of the index of ADL. Gerontologist, 10, 20–30.
Klepin, H.D., Geiger, A.M., Tooze, J.A., Kritchevsky, S.B., Williamson, J.D., Ellis, L.R., . . . Powell, B.L. (2011). The feasibility of inpatient geriatric assessment for older adults receiving induction chemotherapy for acute myelogenous leukemia. Journal of the American Geriatrics Society, 59, 1837–1846. doi:10.1111/j.1532 -5415.2011.03614.x
Klepin, H.D., Geiger, A.M., Tooze, J.A., Kritchevsky, S.B., Williamson, J.D., Pardee, T.S., . . . Powell, B.L. (2013). Geriatric assessment predicts survival for older adults receiving induction chemotherapy for acute myelogenous leukemia. Blood, 121, 4287–4294. doi:10.1182/blood-2012-12-471680
Koroukian, S.M., Bakaki, P.M., Schluchter, M.D., & Owusu, C. (2011). Treatment and survival patterns in relation to multimorbidity in patients with locoregional breast and colorectal cancer. Journal of Geriatric Oncology, 2, 200–208. doi:10.1016/j.jgo.2011.02.004
Kristjansson, S.R., Nesbakken, A., Jordhøy, M.S., Skovlund, E., Audisio, R.A., Johannessen, H.O., . . . Wyller, T.B. (2010). Comprehensive geriatric assessment can predict complications in elderly patients after elective surgery for colorectal cancer: A prospective observational cohort study. Critical Reviews in Oncology/Hematology, 76, 208–217. doi:10.1016/j.critrevonc.2009.11.002
Lawton, M.P., & Brody, E.M. (1969). Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist, 9, 179–186.
Lee, J.H., Fulp, W., Wells, K.J., Meade, C.D., Calcano, E., & Roetzheim, R. (2013). Patient navigation and time to diagnostic resolution: Results for a cluster randomized trial evaluating the efficacy of patient navigation among patients with breast cancer screening abnormalities, Tampa, FL. PLOS One, 8, e74542. doi:10.1371/journal .pone.0074542
Lichtman, S.M., Balducci, L., & Aapro, M. (2007). Geriatric oncology: A field coming of age. Journal of Clinical Oncology, 25, 1821–1823. doi:10.1200/JCO.2007.10.6567
Liu, J.J., & Extermann, M. (2012). Comprehensive geriatric assessment and its clinical impact in oncology. Clinics in Geriatric Medicine, 28, 19–31. doi:10.1016/j.cger.2011.10.001
Lynch, M.P., Marcone, D., & Kagan, S.H. (2007). Developing a multidisciplinary geriatric oncology program in a community cancer center. Clinical Journal of Oncology Nursing, 11, 929–933. doi:10.1188/07.CJON.929-933
Marenco, D., Marinello, R., Berruti, A., Gaspari, F., Stasi, M.F., Rosato, R., . . . Ciccone, G. (2008). Multidimensional geriatric assessment in treatment decision in elderly cancer patients: 6-year experience in an outpatient geriatric oncology service. Critical Reviews in Oncology/Hematology, 68, 157–164. doi:10.1016/j .critrevonc.2008.07.003
McNeil, C. (2013). Geriatric oncology clinics on the rise. Journal of the National Cancer Institute, 105, 585–586. doi:10.1093/jnci/djt104
Mellor, M.J., Davis, K.D., & Capello, C.F. (1997). Stages of development in the life of an academic interdisciplinary team in geriatrics. Gerontology and Geriatrics Education, 18, 3–36. doi:10.1300/J021v18n02_02
Meriggi, F., Andreis, F., Premi, V., Liborio, N., Codignola, C., Mazzocchi, M., . . . Zaniboni, A. (2014). Assessing cancer caregivers’ needs for an early targeted psychosocial support project: The experience of the oncology department of the Poliambulanza Foundation. Palliative and Supportive Care, 1–9. Advance online publication. doi:10.1017/s1478951514000753
Morin, T., Lanièce, I., Desbois, A., Amiard, S., Gavazzi, G., & Couturier, P. (2012). Evaluation of adherence to recommendations within 3 months after comprehensive geriatric assessment by an inpatient geriatric consultation team. Gériatrie et Psychologie Neuropsychiatrie du Vieillissement, 10, 285–293. doi:10.1684/pnv.2012.0359
National Cancer Institute. (2015). SEER stat fact sheets: All cancer sites. Retrieved from http://seer.cancer.gov/statfacts/html/all.html
Overcash, J.A., & Beckstead, J. (2008). Predicting falls in older patients using components of a comprehensive geriatric assessment. Clinical Journal of Oncology Nursing, 12, 941–949. doi:10 .1188/08.CJON.941-949
Overcash, J.A., Beckstead, J., Moody, L., Extermann, M., & Cobb, S. (2006). The abbreviated comprehensive geriatric assessment (aCGA) for use in the older cancer patient as a prescreen: Scoring and interpretation. Critical Reviews in Oncology/Hematology, 59, 205–210. doi:10.1016/j.critrevonc.2006.04.003
Pieters, H.C., Heilemann, M.V., Grant, M., & Maly, R.C. (2011). Older women’s reflections on accessing care across their breast cancer trajectory: Navigating beyond the triple barriers. Oncology Nursing Forum, 38, 175–184. doi:10.1188/11.ONF.175-184
Pinto, A.C., Ferreira-Santos, F., Lago, L.D., de Azambuja, E., Pimentel, F.L., Piccart-Gebhart, M., & Razavi, D. (2014). Information perception, wishes, and satisfaction in ambulatory cancer patients under active treatment: Patient-reported outcomes with QLQ-INFO25. Ecancermedicalscience, 8, 425. doi:10.3332/ecancer.2014.425
Pisu, M., Martin, M.Y., Shewchuk, R., & Meneses, K. (2014). Dealing with the financial burden of cancer: Perspectives of older breast cancer survivors. Supportive Care in Cancer, 22, 3045–3052. doi:10.1007/s00520-014-2298-9
Podsiadlo, D., & Richardson, S. (1991). The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. Journal of the American Geriatrics Society, 39, 142–148. doi:10.1111/ j.1532-5415.1991.tb01616.x
Sattar, S., Alibhai, S.M., Wildiers, H., & Puts, M.T. (2014). How to implement a geriatric assessment in your clinical practice. Oncologist, 19, 1056–1068. doi:10.1634/theoncologist.2014-0180
Schulz, R., & Beach, S.R. (1999). Caregiving as a risk factor for mortality: The Caregiver Health Effects Study. JAMA, 282, 2215–2219. doi:10.1001/jama.282.23.2215
Sherman, F.T. (2008). The patient-caregiver dyad: It takes two to tango! Geriatrics, 63, 13–14.
Simcock, R., & Heaford, A. (2012). Costs of multidisciplinary teams in cancer are small in relation to benefits. BMJ, 344, e3700. doi:10.1136/bmj.e3700
Stanton, M.W. (2006). The high concentration of U.S. health care expenditures. Retrieved from http://archive.ahrq.gov/research/findings/factsheets/costs/expriach/exp…
Stijnen, M.M., Van Hoof, M.S., Wijnands-Hoekstra, I.Y., Guldemond-Hecker, Y., Duimel-Peeters, I.G., Vrijhoef, H.J., & Jansen, M.W. (2014). Detected health and well-being problems following comprehensive geriatric assessment during a home visit among community-dwelling older people: Who benefits most? Family Practice, 31, 333–340. doi:10.1093/fampra/cmu015
Tremblay, D., Charlebois, K., Terret, C., Joannette, S., & Latreille, J. (2012). Integrated oncogeriatric approach: A systematic review of the literature using concept analysis. BMJ Open, 2, e001483. doi:10.1136/bmjopen-2012-001483
Tsai, H.T., Pfeiffer, R.M., Warren, J., Wilson, W., & Landgren, O. (2015). The effects of cardiovascular disease on the clinical outcome of elderly patients with diffuse large b-cell lymphoma. Leukemia and Lymphoma, 56, 682–687. doi:10.3109/10428194.2014.921914
Tucci, A., Ferrari, S., Bottelli, C., Borlenghi, E., Drera, M., & Rossi, G. (2009). A comprehensive geriatric assessment is more effective than clinical judgment to identify elderly diffuse large cell lymphoma patients who benefit from aggressive therapy. Cancer, 115, 4547–4553. doi:10.1002/cncr.24490
Ulrich, C.M., Wallen, G.R., Feister, A., & Grady, C. (2005). Respondent burden in clinical research: When are we asking too much of subjects? IRB, 27, 17–20. doi:10.2307/3563957
U.S. Department of Health and Human Services. (2014). Health, United States, 2013. With special feature on prescription drugs. Retrieved from http://www.cdc.gov/nchs/data/hus/hus13.pdf
van de Water, W., Bastiaannet, E., Egan, K.M., de Craen, A.J., Westendorp, R.G., Balducci, L., . . . Extermann, M. (2014). Management of primary metastatic breast cancer in elderly patients—An international comparison of oncogeriatric versus standard care. Journal of Geriatric Oncology, 5, 252–259. doi:10.1016/j.jgo.2014.02.005
Vandewoude, M. (2010). Nutritional assessment in geriatric cancer patients. Supportive Care in Cancer, 18(Suppl. 2), S51–S56. doi:10.1007/s00520-009-0755-7
Vellas, B., Guigoz, Y., Baumgartner, M., Garry, P.J., Lauque, S., & Albarede, J.L. (2000). Relationships between nutritional markers and the Mini-Nutritional Assessment in 155 older persons. Journal of the American Geriatrics Society, 48, 1300–1309. doi:10.1111/j.1532-5415.2000.tb02605.x
Wildes, T.M., Ruwe, A.P., Fournier, C., Gao, F., Carson, K.R., Piccirillo, J.F., . . . Colditz, G.A. (2013). Geriatric assessment is associated with completion of chemotherapy, toxicity, and survival in older adults with cancer. Journal of Geriatric Oncology, 4, 227–234. doi:10.1016/j.jgo.2013.02.002
Williams, G.R., Deal, A.M., Jolly, T.A., Alston, S.M., Gordon, B.B., Dixon, S.A., . . . Muss, H.B. (2014). Feasibility of geriatric assessment in community oncology clinics. Journal of Geriatric Oncology, 5, 245–251. doi:10.1016/j.jgo.2014.03.001